
Grief & Loss
Loss changes everything: your identity, your faith, the future you expected. Grief counselling in Victoria helps you carry the weight and honour what you lost.
Grief & Loss
A short 15-minute call to discuss your goals, no commitment.
Can counselling help with grief?
Yes. Grief is not a problem to solve or a timeline to finish; it is love with nowhere to go. With support it softens over time, and counselling helps you carry the loss while honouring what you miss. Introspectus Counselling offers grief counselling with Sean Lewis, a Canadian Certified Counsellor, in Colwood, BC and online across BC.
Page Navigation

What are the signs of grief?
Common experiences of grief and loss
If you are reading this, you might recognise these experiences:
The Disorientation: Your sense of identity has been shattered. You don’t know who you are without what you’ve lost.
The Ambush: Grief hits in unpredictable waves; triggered by a song, a smell, or absolutely nothing at all. You thought you were doing better, and then suddenly you aren’t.
The Isolation: People offer platitudes (“At least they aren’t suffering”) that make you feel more alone. You feel like you are grieving in a world that just wants you to “move on.”
The Guilt: You feel guilty for laughing, or for having a good day. Or you replay the past, convinced the loss is somehow your fault.
The Absence: There is a physical hole where something or someone used to be. You cannot imagine how to build a life around this emptiness.
Why does grief feel so heavy?
Why grief doesn’t follow the rules you were given
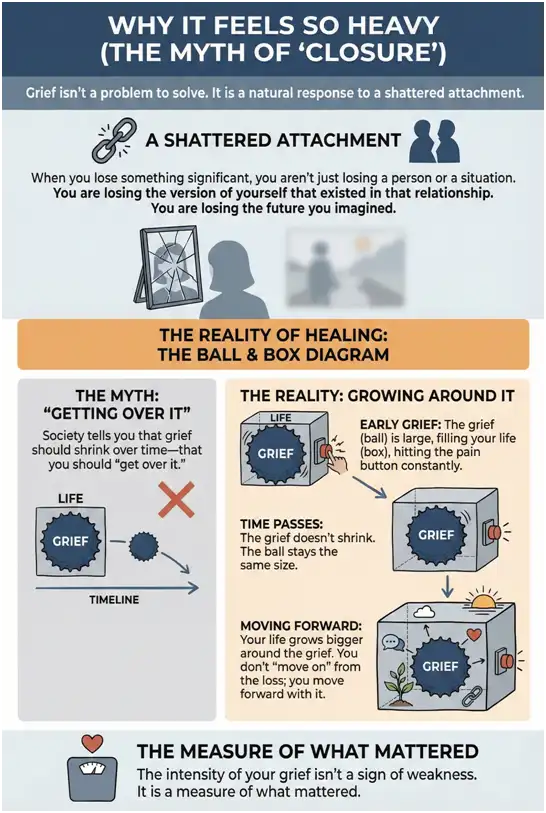
When you lose something significant, you aren’t just losing a person or a situation. You are losing the version of yourself that existed in that relationship. You are losing the future you imagined.
Society tells you that grief should shrink over time; that you should “get over it.” But real grief doesn’t shrink.
The Reality of Healing: The grief doesn’t necessarily get smaller. Instead, your life grows bigger around it. You don’t “move on” from the loss; you move forward with it.
The intensity of your grief isn’t a sign of weakness. It is a measure of what mattered.

How does grief counselling work?
How we work with grief in session
1. The Container (Safety First)
We start by making room for grief exactly as it shows up; messy, contradictory, and non-linear. There is no timeline here. You don’t have to “perform” wellness for me.
2. Continuing Bonds
We don’t aim to sever the connection to what you lost. We aim to find a new way to connect. This might look like ritual, remembrance, or narrative work; finding ways to honour what was lost and integrate its influence into your ongoing life. Grief also lives in your body; we use mindfulness practices to process what’s stored physically.
3. Meaning Reconstruction
Loss often shatters our assumptions about the world (“Life is fair,” “Hard work pays off”). We work to rebuild a worldview that can hold both the reality of the loss and the possibility of joy. We answer the hard question: Who am I now?
This work includes navigating difficult dates, creating personal rituals, and discovering what growth looks like after loss; not in a forced “everything happens for a reason” way, but genuinely exploring what matters now.

Ready to Carry This Differently?
Grief can feel like it will swallow you whole. Let's find a way to honour your loss without being consumed by it.
A short 15-minute call to discuss your goals, no commitment.
What does healing from grief look like?
Healing doesn't mean the sadness disappears. It means the grief becomes something you can carry, rather than something that crushes you.
The Timeline
At first, we just focus on getting through the day. We build structure to keep you functioning.
The "Waves"
You will learn to ride the waves of grief rather than fighting the current.
The Result
You won't "get over" significant loss. But you will develop the capacity to hold both grief and life - to honour the past while finding pockets of meaning and connection in the present.
Get Your Free Letter Worksheet
A gentle, guided letter to the one you lost; a way to stay connected, not say goodbye.
Frequently Asked Questions About Grief Counselling
How long should grief last? Is there a timeline for getting over a loss?
There is no universal timeline for grief. Most people experience intense grief in the first few months, with noticeable improvement within 6-12 months, but grief never fully “ends”; you learn to carry it differently.
Grief becomes concerning when intense, disabling symptoms persist beyond 6-12 months without improvement, preventing you from functioning at work or maintaining relationships. This may indicate prolonged grief disorder, which affects 5-15% of bereaved people and responds well to specialized counselling.
Elena’s experience (fictional example for educational purposes): Six months after her mother died suddenly, she was still crying daily and unable to work. Friends said “it’s been six months; you should be over it.” In counselling, she learned her grief wasn’t “wrong”; it had become complicated and needed support. With therapy, she gradually re-engaged with life while honouring her mother’s memory.
Wondering if your grief needs support? book a free consultation to explore grief counselling.
Evidence-Based Practice References
Bonanno, G. A. (2009). The other side of sadness: What the new science of bereavement tells us about life after loss. Basic Books.
Ivers, N. N., Johnson, D. A., Casares, D. R., Lonn, M. R., Duffey, T., & Haberstroh, S. (2024). Understanding prolonged grief from an existential counselling perspective. Journal of Counselling & Development, 102(3), 370-381. https://doi.org/10.1002/jcad.12518
Prigerson, H. G., & Maciejewski, P. K. (2024). Prolonged grief disorder: Detection, diagnosis, and approaches to intervention. World Psychiatry, 23(3), 361-362. https://doi.org/10.1002/wps.21228
What is grief, and how is it different from depression or sadness?
Grief is yearning for the deceased with self-esteem preserved; depression involves feelings of worthlessness and self-criticism.
Grief: Focus is loss of the “other” (person you loved). Emotions: yearning, longing, sadness, missing them. Self-esteem intact even while deeply sad. Symptoms typically diminish over time.
Depression: Focus is loss of self, personal inadequacy. Emotions: hopelessness, emptiness, pervasive negative mood. Low self-esteem; thoughts of “I’m worthless.” Symptoms persist without treatment.
Maria and Anna’s different experiences (fictional example for educational purposes): After Maria’s father died, she felt overwhelming sadness and thought constantly about memories they shared, but didn’t feel worthless. Her grief was normal. Her friend Anna, after losing her mother, began believing “I’m a terrible daughter; I don’t deserve to be happy.” Anna’s self-criticism indicated depression had developed alongside grief.
They can co-occur, requiring treatment for both.
Unsure if experiencing grief, depression, or both? book a free consultation for clarity and support.
Evidence-Based Practice References
Zisook, S., & Shear, K. (2009). Grief and bereavement: What psychiatrists need to know. World Psychiatry, 8(2), 67-74. https://doi.org/10.1002/j.2051-5545.2009.tb00217.x
Is it normal to feel numb, empty, or unable to cry after someone dies?
Yes. Numbness, emotional flatness, and inability to cry are completely normal early grief reactions, protective responses that help you absorb devastating news gradually.
Numbness is a shock response that typically lasts days to weeks. Some people never cry when grieving and express loss through anger, restlessness, or physical activity. Crying is not the only valid expression of grief.
Mark’s delayed response (fictional example for educational purposes): After his son died, Mark felt nothing. He organized the funeral, answered condolences, and returned to work, all while feeling emotionally dead inside. He worried he was heartless. Two months later, while doing laundry, he found his son’s shirt and collapsed crying. The numbness had simply been delaying the full emotional impact until he could handle it.
Prolonged numbness (months without emotional connection) can indicate avoidance requiring support.
Concerned about prolonged numbness? book a free consultation to explore support.
Evidence-Based Practice References
Zisook, S., & Shear, K. (2009). Grief and bereavement: What psychiatrists need to know. World Psychiatry, 8(2), 67-74. https://doi.org/10.1002/j.2051-5545.2009.tb00217.x
When should I seek grief counselling? Is my grief "bad enough" to need professional help?
You don’t have to be in crisis to benefit from grief counselling. Seek help if experiencing: sudden or traumatic death; loss of a child or spouse; intense grief beyond 6-12 months; complete inability to accept the death; severe functional impairment (cannot work, maintain relationships, care for yourself); constant distress with no relief; or suicidal thoughts.
James’s story (fictional example for educational purposes): His father died of cancer. For three months, he cried often and struggled to concentrate at work. He worried something was wrong with him. In counselling, he learned his grief was entirely normal, but having support helped him process the loss more effectively. He said, “I didn’t need to be ‘broken’ to benefit.”
Research shows grief counselling is most effective for high-risk circumstances and complicated grief symptoms.
Crisis Support: Vancouver Island Crisis Line 1-888-494-3888 (24/7) | 988 Suicide Helpline | 911 immediate danger
Evidence-Based Practice References
Crunk, A. E., Burke, L. A., & Robinson, E. H. (2017). Complicated grief: An evolving theoretical landscape. Journal of Counselling & Development, 95(2), 226-233. https://doi.org/10.1002/jcad.12134
Schut, H., Stroebe, M., van den Bout, J., & Terheggen, M. (2001). The efficacy of bereavement interventions: Determining who benefits. In M. S. Stroebe, R. O. Hansson, W. Stroebe, & H. Schut (Eds.), Handbook of bereavement research: Consequences, coping, and care (pp. 705-737). American Psychological Association.
How can grief counselling help me when nothing can bring the person back?
Therapy can’t bring the person back, but grief counselling uses specific techniques to help you carry the loss while re-engaging with life.
The concrete work we do:
Acceptance work: We practice saying aloud “they died” and sitting with the emotional response, gradually building your capacity to hold this reality without collapsing. You might write letters acknowledging what you’ve lost, visit meaningful places you’ve avoided, or handle belongings you’ve left untouched.
Cognitive restructuring: We identify and challenge unhelpful beliefs (“I don’t deserve happiness without them,” “Moving forward means forgetting them”). You’ll gather evidence for alternative perspectives and test new beliefs through behavioural experiments.
Meaning-making: We explore questions like “What did this relationship teach me?” and “How can I honour them while living?” You might create rituals, reframe the relationship as ongoing rather than ended, or find purpose in advocacy or helping others.
Tom’s transformation (fictional example for educational purposes): After his wife died, he left her coffee mug out every morning. In counselling, he didn’t “let go”, through exposure work, he gradually touched her belongings, visited their favorite places, and practiced imaginal conversations with her. Through values work, he reconnected with his children and returned to hobbies. He said, “Therapy didn’t erase my grief. It taught me I could love her and still have a life.”
Wondering how counselling could help? book a free consultation to explore grief support.
Evidence-Based Practice References
Glickman, K., Shear, M. K., & Wall, M. M. (2016). Mediators of outcome in complicated grief treatment. Journal of Clinical Psychology, 73(7), 817-828. https://doi.org/10.1002/jclp.22384
Ivers, N. N., Johnson, D. A., Casares, D. R., Lonn, M. R., Duffey, T., & Haberstroh, S. (2024). Understanding prolonged grief from an existential counselling perspective. Journal of Counselling & Development, 102(3), 370-381. https://doi.org/10.1002/jcad.12518
How do I know if my grief has become complicated grief or prolonged grief disorder?
Prolonged grief disorder is diagnosed when intense, disabling grief persists beyond 6-12 months with significant functional impairment. It affects 5-15% of bereaved people and responds well to specialized counselling.
Key signs: Persistent yearning for the deceased most of the day; preoccupation with thoughts making it difficult to focus; complete inability to accept the death; severe functional impairment (cannot work, maintain relationships, care for self); constant distress with no relief; life feels meaningless without them.
Specialized treatment approach: Prolonged grief disorder therapy combines acceptance work (gradually approaching avoided reminders), imaginal conversations (structured dialogue with the deceased to process unfinished business), cognitive restructuring of beliefs about the death, and restoration-oriented activities (re-engaging with life, relationships, and future goals). Treatment typically runs 12-16 sessions with specific homework between sessions.
Susan’s experience (fictional example for educational purposes): Fourteen months after her daughter’s death, Susan was unable to work and spent hours staring at photos. She met criteria for prolonged grief disorder. In therapy, she practiced imaginal conversations with her daughter, gradually visited meaningful places she’d avoided, and challenged her belief that living meant betraying her daughter’s memory. After 14 sessions, she returned to work and re-engaged with her grandchildren.
Evidence-Based Practice References
Prigerson, H. G., & Maciejewski, P. K. (2024). Prolonged grief disorder: Detection, diagnosis, and approaches to intervention. World Psychiatry, 23(3), 361-362. https://doi.org/10.1002/wps.21228
Shear, M. K., Wang, Y., Skritskaya, N., Duan, N., Mauro, C., & Ghesquiere, A. (2014). Treatment of complicated grief in elderly persons: A randomized clinical trial. JAMA Psychiatry, 71(11), 1287-1295. https://doi.org/10.1001/jamapsychiatry.2014.1242
What should I expect in my first grief counselling session?
Your first session focuses on understanding your loss and building safety, not forcing you to process feelings before you’re ready. You control what you share.
The assessment process: We’ll explore who you lost, your relationship with them, circumstances of the death, how grief is affecting you (sleep, appetite, concentration, work, relationships), current support systems, and any concerning symptoms like suicidal thoughts or complete inability to function. This isn’t interrogation, it’s collaborative information-gathering so we can determine what help you need most.
Goal-setting and planning: Together, we’ll identify 2-3 specific goals (like “return to work,” “sleep through the night,” or “stop avoiding reminders”) and discuss which therapeutic approaches fit your needs, whether that’s Acceptance and Commitment Therapy, exposure work with avoided situations, or meaning-making exercises.
Sarah’s experience (fictional example for educational purposes): She arrived worried she’d be forced to “let go.” Instead, we spent the hour understanding her relationship with her husband who died, how his death had affected her, and what she needed most. She left saying, “I expected to be pushed. Instead, I felt heard.”
Ready to take the first step? book a free consultation in Victoria, Langford, Saanich, Westshore, or Sooke.
Evidence-Based Practice References
Zisook, S., & Shear, K. (2009). Grief and bereavement: What psychiatrists need to know. World Psychiatry, 8(2), 67-74. https://doi.org/10.1002/j.2051-5545.2009.tb00217.x
Is grief counselling different from regular therapy, and which do I need?
Grief counselling is specialized support using specific techniques for loss and bereavement. Regular therapy addresses broader mental health concerns.
What happens in grief counselling: Sessions focus on processing the reality of death through exposure exercises (visiting avoided places, handling belongings, reviewing photos), restructuring beliefs about the loss (“moving forward means forgetting them”), practicing imaginal conversations to address unfinished business, identifying how you can honour the deceased while living, and taking values-based action toward re-engagement with life. Homework between sessions might include visiting the grave, writing letters to the deceased, or resuming one avoided activity weekly.
What happens in regular therapy: Broader assessment of life patterns, childhood experiences, relationship dynamics, core beliefs formed long before the loss, and general coping skills. Less focus on the specific death; more focus on overall functioning and long-term patterns.
Rachel’s journey (fictional example for educational purposes): After her mother’s death, she sought grief counselling. Six sessions helped her process the loss through exposure work and meaning-making. Later, when she noticed persistent anxiety and relationship patterns unrelated to the loss, she transitioned to general therapy to address these broader concerns.
Unsure which you need? book a free consultation and we’ll determine the best approach together.
Evidence-Based Practice References
Pistrang, N., Barker, C., & Humphreys, K. (2008). Mutual help groups for mental health problems: A review of effectiveness studies. American Journal of Community Psychology, 42(1-2), 110-121. https://doi.org/10.1007/s10464-008-9181-0
Schut, H., Stroebe, M., van den Bout, J., & Terheggen, M. (2001). The efficacy of bereavement interventions: Determining who benefits. In M. S. Stroebe, R. O. Hansson, W. Stroebe, & H. Schut (Eds.), Handbook of bereavement research: Consequences, coping, and care (pp. 705-737). American Psychological Association.
How much does grief counselling cost, and are there affordable or free options?
Sessions cost $150 (50 minutes). Most BC extended health insurance covers 80-100% of fees with a Canadian Certified Counsellor (CCC). Many pay $15-$40/session out-of-pocket.
Payment: You pay at service; I provide receipts you submit to insurer. Most reimburse within 1-2 weeks. Check coverage: ask your insurer “Do you cover Canadian Certified Counsellors?”
Robert’s discovery (fictional example for educational purposes): After his wife’s death, Robert assumed he couldn’t afford counselling. He called his insurance and discovered $2,500 annual coverage at 90% reimbursement, meaning he paid $15/session out-of-pocket. He said, “I was suffering unnecessarily because I thought I couldn’t afford help.”
Free options: Hospice Victoria (free bereavement groups); Victoria Hospice Grief Support (telephone/group); Canadian Virtual Hospice (online resources at virtualhospice.ca); Employee Assistance Programs (EAP: 3-8 free sessions through employer).
Payment plans or sliding scale available for financial hardship.
Ready to use your benefits? book a free consultation and I’ll provide receipts for reimbursement.
Evidence-Based Practice References
BC Association of Clinical Counsellors. (n.d.). Registered clinical counsellor designation. https://bc-counsellors.org/counsellors/
Canadian Counselling and Psychotherapy Association. (n.d.). Canadian Certified Counsellor (CCC) designation. https://www.ccpa-accp.ca/certification/
Is it normal to feel happy, laugh, or have moments of joy while grieving?
Yes. Experiencing happiness, laughter, and joy while grieving is completely normal, and healthy. Grief and positive emotions can coexist; feeling joy doesn’t mean you’ve forgotten or are “over” your loss.
Research shows most bereaved people are resilient, experiencing sadness alongside functioning and moments of positive emotion. Grief comes in waves; intense sadness alternates with periods of calm or even joy. Positive emotions are adaptive, providing psychological breaks that make grief bearable.
How therapy addresses guilt about joy: In counselling, we identify the specific thought driving your guilt (often “If I’m happy, it means I didn’t love them enough”). We examine evidence for and against this belief, explore whether the deceased would want you to suffer forever, and practice behavioural experiments, allowing yourself one moment of joy and observing what actually happens (spoiler: you don’t forget them). You might create permission statements like “I can miss them deeply and still laugh with my children” and practice saying these aloud when guilt arises.
Linda’s guilt (fictional example for educational purposes): After her husband’s death, Linda felt guilty every time she laughed. In counselling, she examined her belief that “joy means I’ve moved on.” She realized her husband would want her to laugh. She practiced allowing joy without immediately suppressing it, eventually realizing, “He would want me to laugh again.”
Struggling with guilt about feeling joy? book a free consultation to explore carrying grief alongside living.
Evidence-Based Practice References
Bonanno, G. A. (2009). The other side of sadness: What the new science of bereavement tells us about life after loss. Basic Books.
Bonanno, G. A., & Kaltman, S. (1999). Toward an integrative perspective on bereavement. Psychological Bulletin, 125(6), 760-776. https://doi.org/10.1037/0033-2909.125.6.760
Are the "five stages of grief" a real process everyone goes through?
No. The “five stages” (denial, anger, bargaining, depression, acceptance) are not universal, and most people don’t experience them in order, or at all.
Elisabeth Kubler-Ross described these stages for dying patients facing their own death in 1969, not for bereaved people. Research shows grief doesn’t follow predictable stages; not everyone experiences all five emotions; stages don’t occur in order; some never experience certain “stages.”
Maya’s confusion (fictional example for educational purposes): After her father’s death, Maya expected to go through the “five stages.” When she didn’t feel anger or bargaining, she worried she was grieving wrong. In counselling, she learned grief is unique for everyone. Her grief involved mostly sadness, yearning, and gradual acceptance, no prescribed stages required.
Stage models invalidate individual experiences (“I should be in acceptance”), create pressure to “progress,” and oversimplify complex grief. Grief is individual, influenced by your relationship, personality, culture, and circumstances.
Ignore anyone saying you’re “in denial” or “should be further along.”
Evidence-Based Practice References
Kubler-Ross, E. (1969). On death and dying. Macmillan.
Maciejewski, P. K., Zhang, B., Block, S. D., & Prigerson, H. G. (2007). An empirical examination of the stage theory of grief. JAMA, 297(7), 716-723. https://doi.org/10.1001/jama.297.7.716
Which kinds of grief and loss do you support?
We support the full range of grief and loss, including bereavement, anticipatory grief, complicated grief, and non-death losses like divorce or a major life change.
Normal Grief
Normal Grief (also called uncomplicated grief or bereavement) is the natural emotional response to losing someone or something important to you. It can include waves of sadness, anger, confusion, and even relief, all of which are valid. You do not need to be “stuck” or in crisis to benefit from grief therapy; working with a therapist during Normal Grief gives you a supported space to process what you are feeling at your own pace and in your own way.
Prolonged Grief Disorder (sometimes referred to as complicated grief or persistent complex bereavement disorder) is recognised when intense grief persists well beyond what might be expected and significantly interferes with your ability to function in daily life. You may find yourself unable to accept the loss, feeling emotionally numb, or withdrawing from relationships and activities that once mattered. Prolonged Grief Disorder is a clinical condition that responds to targeted therapeutic approaches; it is not a sign of weakness or an inability to “move on.”
Therapeutic Approaches
ACT helps you make room for the pain of grief without being consumed by it. Rather than trying to eliminate sadness or force yourself to “get over it,” you learn to hold difficult emotions with openness while reconnecting with the values and relationships that still give your life meaning.
Cognitive Behavioural Therapy (CBT)
Cognitive Behavioural Therapy (CBT) addresses unhelpful thought patterns that can deepen grief: beliefs like “I should have done more,” “I will never feel normal again,” or guilt about moments of happiness. CBT provides structured tools to gently examine these thoughts and develop more balanced perspectives, which is especially helpful when grief becomes intertwined with anxiety or depression.
Narrative Therapy invites you to tell the story of your relationship with the person you lost and explore how that story shapes who you are now. Through this process you can honour what the relationship meant, find language for experiences that feel wordless, and gradually integrate the loss into a broader life narrative rather than being defined by it.
Mindfulness-Based Therapy teaches you to be present with grief rather than bracing against it or being swept away. For many people, grief comes in unpredictable waves, mindfulness skills help you notice what is happening in your body and mind, respond with self-compassion rather than judgment, and build tolerance for the discomfort that accompanies loss.
Compassion-Focused Therapy (CFT)
Compassion-Focused Therapy (CFT) is particularly valuable in grief work because loss often triggers harsh self-criticism: you may blame yourself, feel ashamed of how you are coping, or believe you do not deserve support. CFT helps you develop a warmer, more compassionate relationship with yourself so you can grieve without the added burden of self-judgment.
Grief Therapy in Victoria | Loss Doesn’t Follow a Timeline
Grief does not follow a schedule. Maybe grief hits out of nowhere, months after you thought you were fine. Maybe you cannot cry even though you know you should feel something. Maybe you are grieving but also relieved, and nobody told you that was allowed. Maybe it has been a year and you are still not over it, and the people around you have stopped asking.
Some losses the world does not even recognise; grief after divorce, the loss of a pet that others dismiss, a miscarriage no one talks about, or the quiet devastation of disenfranchised grief where your mourning has no socially acceptable container.
I’m Sean Lewis, a Canadian Certified Counsellor (CCC #11252849) with the CCPA. I have ten years of pastoral ministry behind me, including funerals, end-of-life companionship, and sitting with families navigating anticipatory grief. At the Mustard Seed Street Church in Victoria, loss was constant; loss of housing, relationships, identity, and community. I learned that the textbook stages of grief rarely match what people actually experience.
As a grief therapist in Victoria, BC, I use narrative therapy to help you honour what you have lost, and Acceptance and Commitment Therapy (ACT) to build a path forward that does not require getting over it. Research supports both modalities for complicated grief, anticipatory grief, and bereavement that refuses to follow a predictable timeline.
I offer grief counselling in Colwood, Langford, and the Westshore, with virtual bereavement support across British Columbia. book a free consultation.
Most extended health plans reimburse sessions with a Canadian Certified Counsellor. I hold this designation through the CCPA.