
Intrusive Thoughts & Rumination
Breaking the cycle of sticky thoughts and endless mental loops. ACT-based therapy for intrusive thoughts in Victoria helps you loosen their grip and find relief.
Intrusive Thoughts & Rumination
A short 15-minute call to discuss your goals, no commitment.
Can therapy help with intrusive thoughts?
Yes. Intrusive thoughts are not a sign of who you are or what you secretly want; they are a stuck loop in an anxious brain. Counselling helps you loosen the loop by changing how you respond to the thoughts, not by fighting them. Introspectus Counselling offers support for intrusive thoughts with Sean Lewis, a Canadian Certified Counsellor, in Colwood, BC and online across BC.
Page Navigation

What are the signs of intrusive thoughts and rumination?
Common patterns of intrusive thoughts and rumination
If you are reading this, you might recognise these experiences:
The Sticky Thought: You experience sudden, unwanted thoughts that feel scary, weird, or completely out of character. You worry that having the thought means something terrible about who you are.
The Mental Replay: You endlessly rehash past conversations or mistakes. Your brain won’t let you move on, even when you know ruminating isn’t fixing anything.
The What-If Spiral: Your mind generates endless worst-case scenarios. You try to “think through” every possibility to feel prepared, but the mental rehearsal never brings relief.
The Backfire Effect: The more you try not to think about something, the more it dominates your mind. Pushing thoughts away only makes them stronger.
Checking and Reassurance: You constantly analyse your thoughts to make sure you’re “okay,” or seek reassurance from others. The relief is temporary, and the cycle starts again.
Why does the brain get stuck in loops?
The mechanism that keeps your mind stuck
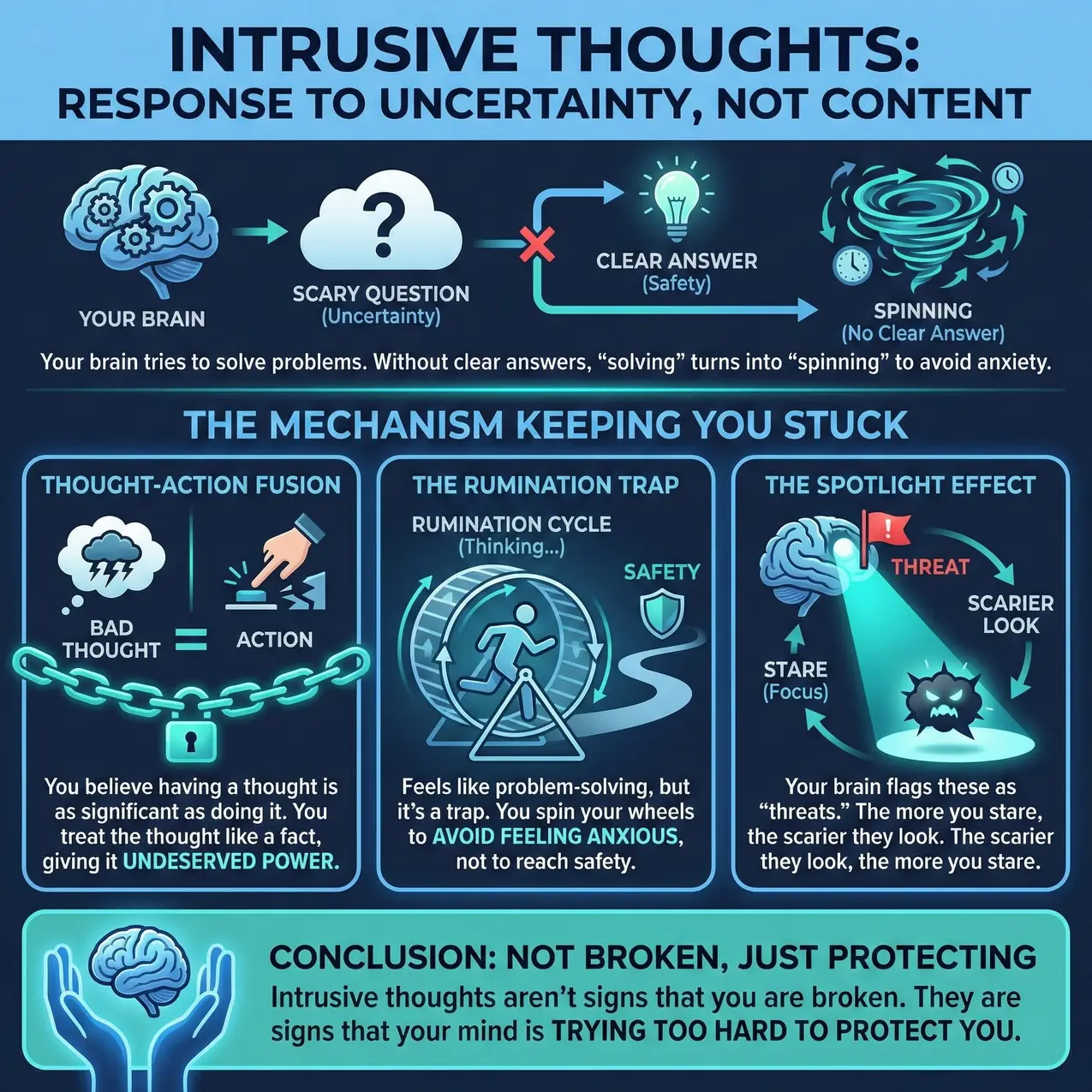
Your brain is designed to solve problems. When it encounters a scary question (“What if I said the wrong thing?” “What does this thought mean about me?”), it tries to think its way to safety. But because these questions don’t have clear answers, the “solving” turns into “spinning.”
Here is the mechanism keeping you stuck:
Fusion: Your mind treats thoughts as if they are facts. Having a scary thought feels the same as doing something scary. This is called fusion; your mind has fused the thought with reality, giving it power it doesn’t deserve.
The Rumination Trap: Rumination feels like problem-solving, but it is actually a trap. You are trying to “think” your way to safety, but you are really just spinning your wheels to avoid feeling anxious.
The Spotlight Effect: Your brain has flagged these thoughts as “threats.” The more you stare at them (focus), the scarier they look. The scarier they look, the more you stare.
The intrusive thoughts aren’t signs that you are broken. They are signs that your mind is trying too hard to protect you.
- Thought-Action Fusion: You believe that having a bad thought is just as significant as doing You treat the thought like a fact, which gives it power it doesn’t deserve.
- The Rumination Trap: Rumination feels like problem-solving, but it is actually a trap. You are trying to “think” your way to safety, but you are really just spinning your wheels to avoid feeling anxious.
- The Spotlight Effect: Your brain has flagged these thoughts as “threats.” The more you stare at them (focus), the scarier they look. The scarier they look, the more you stare.
How does therapy for intrusive thoughts work?

How does therapy for intrusive thoughts work?
If the same thought keeps circling, there is a short way through. This guide to getting out of a thought loop shows a practice that takes about a minute.
How the therapeutic work actually works
We don’t start by trying to eliminate the thoughts; that usually makes them stronger. We start by changing your relationship with them.
1. Mapping the Mechanism
We examine your triggers and your responses (checking, seeking reassurance, suppressing). We identify how the things you do to “cope” are actually keeping the cycle alive.
2. Creating Distance (Cognitive Defusion)
You will learn that thoughts are just thoughts; not facts, not predictions, and not reflections of your character. Think of thoughts like weather passing through the sky. You can notice a storm cloud without becoming the storm. We practise observing the thought (“There is that thought again”) without grabbing onto it.
3. Practising Willingness
For intrusive thoughts, we practise willingness; deliberately allowing a thought to exist without engaging in mental rituals like checking or analysing. This is not about forcing yourself to enjoy the thought. It is about dropping the struggle with it.
The Goal: When you stop fighting the thought, the anxiety peaks and then naturally decreases on its own. Your brain learns that the alarm is false; not because you argued with it, but because you stopped treating it as an emergency.
4. Exiting the Rumination Loop
We work on recognising the exact moment you cross from “productive problem-solving” into “unproductive spinning.” You will learn to redirect your attention to what is actually in front of you; what you can see, hear, and touch right now; rather than arguing with the noise in your head.
Note: I am not here to tell you what to believe. I am here to help you think deeply, feel honestly, and find your own authentic path forward.

Ready to Get Unstuck From the Loop?
Those thoughts are not who you are. Let's learn to let them pass without them taking over.
A short 15-minute call to discuss your goals, no commitment.
What does recovery feel like?
Recovery from intrusive thoughts is realistic, and it feels less like the thoughts disappearing and more like them losing their grip on you. Change here is gradual, and it might feel counterintuitive at first.
Early Shifts
You might first notice that you catch yourself ruminating sooner. The thoughts might not vanish immediately, but your distress about them will decrease.
The Work
Some techniques will feel uncomfortable - like deliberately letting a "bad" thought sit in your mind without pushing it away. This discomfort is part of the process, not a sign of failure.
The Result
You won't become someone who never has unwanted thoughts. But you will develop the capacity to let thoughts pass through without getting stuck on them. The mental static won't control your day.

Get Your Free Defusion Exercise
A short, interactive exercise for stepping back from the thoughts that arrive uninvited, and the loops that will not switch off.
Frequently Asked Questions About Intrusive Thoughts
What is the difference between an intrusive thought and a real desire or urge to act?
An intrusive thought is unwanted, distressing, and goes against your values. A real desire feels natural and aligned with who you are. If a thought horrifies you, it is an intrusive thought, not a secret desire.
The “Radio Station” Analogy
Think of your mind like a radio scanning stations. Most of the time, you’re tuned to your regular station, thoughts that match your values. But sometimes the radio catches a disturbing signal (violence, harm, taboo content). That’s an intrusive thought, not a secret desire.
People with OCD or high anxiety mistakenly believe having the thought means they want to do it.
A Common Example Case Study (Composite scenario for educational purposes):
Michael is driving with his toddler in the backseat. The thought pops up: “What if I just kept driving into oncoming traffic?” His heart races. He grips the wheel tighter. He immediately pulls over, checks on his daughter, and spends 20 minutes trying to figure out “why I would think that.” The horror he feels proves this is an intrusive thought, not a desire.
Why the Thoughts Get Stuck: The Cycle
Intrusive thoughts get stuck because you react to them with fear:
1. The Thought: “What if I drop my baby down the stairs?” 2. The Meaning: “Only a monster would think that.” (Anxiety spikes) 3. The Reaction: You avoid the stairs, check your feelings, and analyse your past 4. The Result: Your brain tags the thought as “dangerous,” guaranteeing it will return
How We Work (ACT & Defusion)
Using Acceptance and Commitment Therapy (ACT), we help you stop fighting the thoughts:
- Defusion: Learn to see thoughts as just mental noise, not facts
- Clarify Values: Intrusive thoughts attack what you love most; if you have intrusive thoughts about harming your family, it’s actually proof of how much you value their safety
- Break Compulsions: Stop analysing, checking, and seeking reassurance
- Tolerate Uncertainty: “What if?” thoughts lose power when you can sit with not knowing for sure
A Note on Safety:
If you’re worried about whether a thought is intrusive, that worry itself is usually proof it’s intrusive; people with genuine harmful intent do not obsess over their thoughts. However, if you have actual plans to harm yourself or others (not horrifying thoughts, but genuine urges), please call the Vancouver Island Crisis Line at 1-888-494-3888 immediately.
As a book a free consultation specializing in anxiety and OCD, I help you recognise intrusive thoughts for what they are: mental noise, not truth.
Ready to break free from the loop? book a free consultation in Greater Victoria (Victoria, Langford, Saanich, Westshore, Sooke).
Evidence-Based Practice References
International OCD Foundation. “What is OCD?” Accessed February 2, 2026. https://iocdf.org/about-ocd/
Abramowitz, J. S., Taylor, S., & McKay, D. “Obsessive-Compulsive Disorder.” The Lancet 374, no. 9688 (2009): 491-499. https://doi.org/10.1016/S0140-6736(09)60240-3
Twohig, M. P., Hayes, S. C., & Masuda, A. “Increasing Willingness to Experience Obsessions: Acceptance and Commitment Therapy as a Treatment for Obsessive-Compulsive Disorder.” Behavior Therapy 37, no. 1 (2006): 3-13. https://doi.org/10.1016/j.beth.2005.02.001
Canadian Counselling and Psychotherapy Association (CCPA). “Code of Ethics (2020).” Article A6 “Respect for Client Autonomy.” Ottawa: CCPA, 2020. https://www.ccpa-accp.ca/wp-content/uploads/2020/05/CCPA-2020-Code-of-Ethics-E-Book-EN.pdf
If I have thoughts about harming someone, does that mean I am a dangerous person?
No. Having intrusive thoughts about harming someone does not mean you are dangerous, and the fact that these thoughts disturb you is strong evidence you wouldn’t act on them. Research shows up to 90% of people experience unwanted, disturbing thoughts at some point; the anxiety you feel about these thoughts actually demonstrates they conflict with your values.
The Critical Distinction
Intrusive thoughts (what you’re likely experiencing):
- Unwanted and distressing; they horrify you
- No actual desire or plans to carry them out
- You’re seeking reassurance because the thoughts clash with who you are
Genuine intent to harm (signs of actual risk):
- Making specific plans or preparations
- Thoughts feel wanted, justified, or acceptable
- No distress about the thoughts; may feel satisfaction
The key difference: If you’re reading this because these thoughts horrify you, that horror is evidence you’re not dangerous.
A Common Pattern Case Study (Composite scenario for educational purposes):
Maria had intrusive images of stabbing her husband while cooking dinner. She immediately hid all the knives in the garage, stopped cooking, and spent hours crying and Googling “am I a psychopath?” Her therapist asked: “Do you want to hurt him?” Maria looked horrified. “Of course not! I love him more than anything. That’s why these thoughts are so terrifying.” The distress proved these were intrusive thoughts, not dangerous impulses.
What’s Actually Happening
You’re likely experiencing harm OCD (obsessive-compulsive disorder with harm obsessions); intrusive, unwanted thoughts about harming others that cause intense anxiety. People with harm OCD are statistically LESS likely to act on violent thoughts than the general population because they find the thoughts so disturbing.
Common examples:
- Thoughts about stabbing or hurting a loved one
- Intrusive images of pushing someone in front of traffic
- Fear of “snapping” and losing control
- Worries about being a pedophile despite no attraction
You’re not alone, and you’re not dangerous. These thoughts are extremely common, deeply distressing, and highly treatable.
How Therapy Helps
Using Acceptance and Commitment Therapy (ACT), therapy helps you:
- Recognise intrusive thoughts as mental noise rather than meaningful information about your character
- Reduce the power of thought-action fusion (the false belief that thinking something makes it more likely to happen)
- Tolerate the anxiety without seeking reassurance or performing mental rituals
- Rebuild trust in yourself as a safe, non-dangerous person
The hard part: Treatment involves facing the thoughts without doing compulsions (reassurance-seeking, mental checking, avoidance). This is terrifying at first but essential for breaking the cycle.
The reality: Harm obsessions respond well to ACT and Exposure and Response Prevention (ERP). Recovery means the thoughts lose their power to control your life.
You’re Not Alone
Thousands of people experience exactly what you’re describing. The shame and secrecy make it worse. Therapy gives you a place to say these thoughts out loud without judgment.
Ready to get help? book a free consultation in Victoria, Langford, Saanich, the Westshore, or Sooke to work on intrusive thoughts and harm obsessions using evidence-based approaches.
Evidence-Based Practice References
Rachman, S., & de Silva, P. “Abnormal and Normal Obsessions.” Behaviour Research and Therapy 16, no. 4 (1978): 233-248. https://doi.org/10.1016/0005-7967(78)90022-0
Twohig, M. P., Hayes, S. C., & Masuda, A. “Increasing Willingness to Experience Obsessions: Acceptance and Commitment Therapy as a Treatment for Obsessive-Compulsive Disorder.” Behavior Therapy 37, no. 1 (2006): 3-13. https://doi.org/10.1016/j.beth.2005.02.001
Shafran, R., Thordarson, D. S., & Rachman, S. “Thought-Action Fusion in Obsessive-Compulsive Disorder.” Journal of Anxiety Disorders 10, no. 5 (1996): 379-391. https://doi.org/10.1016/0887-6185(96)00018-7
How common are intrusive thoughts; am I the only one dealing with this?
You are absolutely not alone. You are not “sick,” and you are not broken.
Research shows that up to 80% of the general population experiences intrusive, unwanted thoughts similar to those seen in obsessive-compulsive disorder (OCD).
The Difference Isn’t Having the Thoughts: It’s the Response
Most people have bizarre, disturbing, or taboo thoughts pop into their minds occasionally:
- “What if I swerved into oncoming traffic?”
- “What if I pushed someone off this ledge?”
- Unwanted sexual or violent images
What separates normal intrusive thoughts to not normal:
- Healthy: “That was weird” -> dismiss it -> move on with their day
- Gain Suppport: “That was weird -> What does this mean about me? -> Am I dangerous? -> I need to figure this out” -> hours of rumination
People with an unhealthy thought pattern interpret these thoughts as personally meaningful to an exaggerated extent, which constitutes a clinical diagnosis, while people with a healthy thought pattern appraise them in a way that doesn’t implicate personal responsibility.
These Themes Are Common (Even the Scary Ones)
Research confirms that taboo or unacceptable thoughts regarding harming oneself or others, morality, incest, pedophilia, sacrilege, sexuality, and violent images occur commonly, yet are frequently misidentified even by trained professionals.
Why Shame Keeps People Isolated
OCD is prevalent in up to 2.3% of the population and frequently experienced as chronic and debilitating. The shame and secrecy surrounding intrusive thoughts keep people isolated. Many clients share that they believed they were “the only person sick enough” to have these thoughts. Discovering how common they are brings immediate relief.
These thoughts are just a symptom, not a reflection of your character. book a free consultation to discuss how specialized OCD therapy in Victoria BC can help.
Evidence-Based Practice References
Johansen, Tore, Wolfgang H. Dittrich, and Umberto Albert. “Cognitive Performance in a Subclinical Obsessive-Compulsive Sample
Cognitive Functions.” Psychiatry Journal 2013, no. 1 (2013). https://doi.org/10.1155/2013/565191
Weinberg, Lauren, Loni A. Martin, Kristin M. Post, and Emily J. Ricketts. “Psychologists’ Diagnostic Accuracy and Treatment Recommendations for Obsessive-Compulsive Disorder.” Journal of Clinical Psychology 81, no. 5 (2025): 324-333. https://doi.org/10.1002/jclp.23775
Why do I have intrusive thoughts about hurting people I love when I would never actually do it?
Your brain generates intrusive thoughts about hurting the people you love most precisely BECAUSE you love them and would never hurt them. The thoughts target what you value most as a way of testing your commitment to protecting them. This is a cruel paradox of harm: the more you care about someone’s safety, the more your anxious brain produces disturbing thoughts about harming them.
Research shows this pattern is extremely common in new parents, caregivers, and people in intimate relationships; the intensity of your distress about these thoughts is actually evidence they conflict with your values.
Case Study (Composite scenario for educational purposes)
Elena had a six-week-old son. While holding him near the stairs, the thought flashed: “What if I just threw him down?” She immediately froze, handed the baby to her partner, and refused to hold him near any heights. She spent nights awake Googling “do I want to hurt my baby?” The fact that she was horrified proved she was a protective mother, not a dangerous one.
Why This Pattern Makes Sense
Your brain’s threat-detection system becomes hypervigilant about protecting people you love. But instead of just scanning for external dangers, anxious brains also generate internal “what if” scenarios. The people who matter most evoke the strongest emotions, so thoughts about them carry more weight and become “stickier.”
Common examples:
- New parents with thoughts about dropping, shaking, or harming their baby during caregiving
- Partners with thoughts about stabbing or violence during intimate moments
- Parents with disturbing thoughts about their children during normal activities
This isn’t about hidden desires. If these thoughts reflected what you actually wanted, you would:
- Feel satisfaction when having them (you don’t)
- Make plans (you don’t)
- Have these thoughts about people you dislike (you don’t; they target people you love)
The pattern reveals: Your intrusive thoughts target your VALUES, not your desires. This is evidence of your moral character, not a threat to it.
How Therapy Helps
Using Acceptance and Commitment Therapy (ACT) and Exposure and Response Prevention (ERP), therapy helps you:
- Understand that disturbing thoughts about loved ones reflect the depth of your care, not hidden danger
- Recognise these thoughts noise rather than meaningful warnings
- Stop the reassurance-seeking and mental checking that maintains the cycle
- Act according to your values (being loving and protective) regardless of what thoughts appear
You’re not a monster; you’re anxious. The people most disturbed by intrusive harm thoughts are the LEAST likely to act on them. Your distress is proof of your values, not evidence against them.
Ready to stop being tormented by these thoughts? book a free consultation in Victoria, Langford, Saanich, the Westshore, or Sooke to work on intrusive harm thoughts using evidence-based approaches.
Evidence-Based Practice References
Abramowitz, J. S., et al. “Obsessive-Compulsive Symptoms in Pregnancy and the Puerperium: A Review of the Literature.” Journal of Anxiety Disorders 17, no. 4 (2003): 461-478. https://doi.org/10.1016/S0887-6185(02)00206-2
Rachman, S. “A Cognitive Theory of Obsessions.” Behaviour Research and Therapy 35, no. 9 (1997): 793-802. https://doi.org/10.1016/S0005-7967(97)00040-5
Twohig, M. P., Hayes, S. C., & Masuda, A. “Increasing Willingness to Experience Obsessions: Acceptance and Commitment Therapy as a Treatment for Obsessive-Compulsive Disorder.” Behavior Therapy 37, no. 1 (2006): 3-13. https://doi.org/10.1016/j.beth.2005.02.001
Shafran, R., Thordarson, D. S., & Rachman, S. “Thought-Action Fusion in Obsessive-Compulsive Disorder.” Journal of Anxiety Disorders 10, no. 5 (1996): 379-391. https://doi.org/10.1016/0887-6185(96)00018-7
What are unwanted sexual intrusive thoughts, and how are they different from actual attraction?
Unwanted sexual intrusive thoughts are distressing images or impulses that pop into your mind against your will. They feel foreign, disturbing, and completely at odds with your values.
The Key Difference: “Dread” vs. “Desire”
Actual sexual attraction feels pleasurable, wanted, and aligned with who you are. Intrusive thoughts, by contrast, cause intense distress and anxiety.
- If it’s attraction: You lean into the thought; it feels exciting or pleasurable
- If it’s OCD: You feel horrified, disgusted, and try desperately to suppress or “figure out” what the thought means
A Common Example Case Study (Composite scenario for educational purposes):
A straight man scrolling Instagram sees a shirtless male celebrity and has the intrusive thought: “What if I’m attracted to him?” His body tenses. He immediately checks for any physical response, analyzes past relationships for “signs,” and spends the evening Googling “am I gay?” The anxiety and rumination prove this is OCD, not attraction.
Why These Thoughts Get Stuck
When a disturbing thought occurs, your brain misinterprets it as a threat. You then engage in mental compulsions (like ruminating, checking your body’s physical response, or seeking reassurance) to reduce the anxiety. Unfortunately, this reaction tells your brain the thought is important, keeping you trapped in the loop.
You Are Not Alone (And You Are Not Your Thoughts)
Research shows that taboo thoughts regarding sexuality, pedophilia, or incest are common in OCD. Yet, a 2025 study found that over one-third (35%) of licensed psychologists incorrectly misdiagnose Sexual Orientation OCD (SO-OCD) because they don’t understand the condition.
These thoughts say nothing about your true desires; they are just sticky mental noise that OCD latches onto.
How We Treat It:
We use Exposure and Response Prevention (ERP) to help you change your relationship with these thoughts, teaching your brain that they are safe to ignore.
Ready to break the cycle of shame? book a free consultation
Evidence-Based Practice References
Weinberg, Lauren, Loni A. Martin, Kristin M. Post, and Emily J. Ricketts. “Psychologists’ Diagnostic Accuracy and Treatment Recommendations for Obsessive-Compulsive Disorder.” Journal of Clinical Psychology 81, no. 5 (2025): 324-333. https://doi.org/10.1002/jclp.23775
When should I seek professional help for intrusive thoughts instead of trying to manage them on my own?
You do not need to wait until you hit “rock bottom” to seek help. If intrusive thoughts are stealing your time, energy, or peace of mind, it is time to reach out.
The “One Hour” Rule
Clinical guidelines suggest seeking therapy if intrusive thoughts consume more than one hour of your day or significantly interfere with your life.
Warning Signs It’s Time for Support:
- Exhaustion: You spend hours analysing the thoughts, trying to “figure them out,” or pushing them away
- Avoidance: You stop doing things you love, or avoid certain people/places because they trigger the thoughts
- Reassurance Seeking: You constantly ask loved ones or Google if you are a “good person” or if you’re going crazy
- Disrupted Presence: You have trouble concentrating at work, school, or during conversations because of the mental noise
A Common Pattern Case Study (Composite scenario for educational purposes):
Sarah stopped watching TV shows with her family because crime dramas triggered intrusive thoughts about harming loved ones. She avoided the kitchen after dinner because seeing knives caused hour-long rumination spirals. She called in sick to work three times last month because she couldn’t concentrate. The thoughts were now controlling her choices.
You Are Not Alone
Research shows that up to 80% of the population experiences bizarre or taboo thoughts. The difference is that OCD brain locks onto them and rings a false alarm. Early intervention with specialized OCD therapy can stop these patterns from becoming entrenched.
Immediate Safety Check:
Intrusive thoughts are usually horrifying to the person having them. However, if you are experiencing a genuine urge or plan to harm yourself or others, please contact the Vancouver Island Crisis Line at 1-888-494-3888 or call 911 immediately.
Ready to get your time back? book a free consultation
Evidence-Based Practice References
American Psychological Association. “Understanding Psychotherapy and How It Works.” Accessed February 2, 2026. https://www.apa.org/topics/psychotherapy/understanding
Johansen, Tore, Wolfgang H. Dittrich, and Umberto Albert. “Cognitive Performance in a Subclinical Obsessive-Compulsive Sample 1: Cognitive Functions.” Psychiatry Journal 2013, no. 1 (2013). https://doi.org/10.1155/2013/565191
Clinical Note: OCD is diagnosed when obsessions/compulsions consume more than 1 hour per day and cause significant impairment.
Is therapy effective for intrusive thoughts and OCD; will I ever truly be free of them?
Yes, therapy works. And no, the goal isn’t to never have another intrusive thought again.
The good news: You can become completely free from the control these thoughts have over you, even if occasional thoughts still pop up.
What “Freedom” Actually Looks Like
Most people imagine recovery means a mind completely scrubbed clean of disturbing thoughts. The reality is better than that: you learn to stop caring when they show up.
- Before treatment: “I had a disturbing thought -> I must analyse it for hours -> I feel tortured”
- After treatment: “I had a disturbing thought -> my brain does that sometimes -> I continue with my day”
The Research on Effectiveness
Exposure and Response Prevention (ERP) is the gold-standard psychotherapeutic intervention for OCD. Research shows that 60-90% of adults with OCD benefit from CBT treatment, experiencing substantial symptom reduction.
A 2024 meta-analysis found that guided self-help cognitive behavioural therapy significantly reduced OCD symptomatology compared to active controls, demonstrating the effectiveness of evidence-based approaches.
What You’ll Gain
- Thoughts lose their “stickiness” and emotional charge
- You stop spending hours ruminating or seeking reassurance
- You can handle uncertainty without performing rituals
- You reclaim time and energy for what actually matters
The goal isn’t thought elimination; it’s freedom from the compulsion to respond to them.
Ready to change your relationship with intrusive thoughts? book a free consultation
Evidence-Based Practice References
Faustino, Diogo, Miguel M. Goncalves, Raquel Braga, Maria Joao Faria, and Joao T. Oliveira. “Exposure and Response Prevention in OCD: A Framework to Capitalize Change.” Journal of Clinical Psychology 81, no. 7 (2025): 643-651. https://doi.org/10.1002/jclp.23797
Polak, Monika, and Nikolaus Tanzer. “Internet-Based Cognitive Behavioural Treatments for Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis.” Clinical Psychology & Psychotherapy 31, no. 3 (2024). https://doi.org/10.1002/cpp.2989
How long does therapy for intrusive thoughts usually take before I notice improvement?
Most people begin noticing relief within 8-12 weeks of consistent, weekly therapy. Meaningful, lasting change typically requires 12-16 sessions, though your timeline depends on three key factors.
What “Improvement” Actually Looks Like
Early wins often include:
- Reduced rumination time: You catch yourself faster and redirect attention
- Increased confidence: You handle triggers without falling apart
- Decreased anxiety: When intrusive thoughts occur, they don’t send you into a spiral
You may still have intrusive thoughts, but they lose their emotional charge and you stop treating them as emergencies.
A Typical Progression:
Week 4: James noticed he could hold his newborn daughter without spending 30 minutes afterward analysing whether he had harmful thoughts. Week 8: He went an entire day without checking Google for reassurance. Week 12: A disturbing thought popped up during a diaper change, and he simply continued changing the diaper. The thought still felt uncomfortable, but it no longer controlled his actions.
Three Factors That Affect Your Timeline
1. Severity & Duration
- Mild to moderate OCD: 8-12 sessions may be sufficient
- Severe OCD or long-standing patterns: 20-30 sessions or longer
- Research shows that although ERP is intended to be short-term (averaging 8-16 weeks), more severe symptom presentations may require a longer course of treatment
2. Between-Session Practice Active homework practice significantly speeds improvement. Patients who expose themselves to triggers during therapy sessions and at home gain maximum benefit from ERP. Treatment typically includes 12-16 weekly sessions complemented by homework assignments between sessions.
3. Treatment Approach Specialized ERP shows faster results than traditional talk therapy. A case study of severe OCD showed clinician-based Y-BOCS scores reduced by 65% after 14 individual 50-minute ERP sessions.
The Three Stages of Recovery
Research shows improvement happens in stages:
1. Learn skills and build tolerance (weeks 1-6) 2. Notice reduced compulsions (weeks 6-12) 3. Intrusive thoughts decrease in frequency and intensity (weeks 12+)
Ready to start your timeline? book a free consultation to create a treatment plan tailored to your specific situation in Victoria BC.
Evidence-Based Practice References
Polak, Monika, and Nikolaus Tanzer. “Internet-Based Cognitive Behavioural Treatments for Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis.” Clinical Psychology & Psychotherapy 31, no. 3 (2024). https://doi.org/10.1002/cpp.2989
Jones, Maree K., Bethany M. Wootton, Luke D. Vaccaro, Iuliana G. Anghelescu, and Samuele Cortese. “The Efficacy of Exposure and Response Prevention for Geriatric Obsessive Compulsive Disorder: A Clinical Case Illustration.” Case Reports in Psychiatry 2012, no. 1 (2012). https://doi.org/10.1155/2012/394603
Jessup, Samantha C., Abbe Mariaskin, and Bunmi O. Olatunji. “Strategies for Optimizing Traditional Exposure and Response Prevention: A Case Study Example in an Adolescent With Contamination-Based OCD.” Journal of Clinical Psychology 81, no. 3 (2024): 182-192. https://doi.org/10.1002/jclp.23758
Gosnell, Hannah L., Anita S. Kablinger, and Daisuke Matsuzawa. “A Case of Cachexia Secondary to Obsessive-Compulsive Disorder.” Case Reports in Psychiatry 2020, no. 1 (2020). https://doi.org/10.1155/2020/5783191
What is the difference between regular talk therapy and specialized OCD or intrusive thought therapy?
Regular talk therapy can sometimes make OCD worse. Traditional therapy often focuses on exploring why you are having a thought and trying to reassure you that the thought isn’t true. For someone with OCD or intrusive thoughts, this accidentally feeds the compulsion to analyse and ruminate.
The Difference in Approach:
- Regular Talk Therapy: “Let’s figure out where this thought comes from and prove it’s not true.” (This keeps you trapped in the debate)
- Specialized OCD Therapy (ERP): “Let’s practice tolerating the discomfort of the thought without arguing with it, until your brain learns it is safe to ignore.”
What is ERP?
We use Exposure and Response Prevention (ERP), the gold-standard treatment for OCD, alongside Acceptance and Commitment Therapy (ACT).
Instead of fighting the thoughts, ERP helps you gradually face the triggers while preventing the compulsive response (like checking, avoiding, or asking for reassurance). Over time, this rewires the brain to stop sending false alarm signals.
Why This Matters
Research demonstrates that when both client and therapist become entrenched in cognitive restructuring (trying to rationally counter obsessive thoughts through logic), it can inadvertently reinforce compulsive patterns by providing temporary reassurance rather than promoting long-term cognitive flexibility.
At our Victoria BC practice, the goal is not to analyse the mental noise, but to help you live a life based on your values, even when the noise is present.
Tired of arguing with your thoughts? book a free consultation
Evidence-Based Practice References
Faustino, Diogo, Miguel M. Goncalves, Raquel Braga, Maria Joao Faria, and Joao T. Oliveira. “Exposure and Response Prevention in OCD: A Framework to Capitalize Change.” Journal of Clinical Psychology 81, no. 7 (2025): 643-651. https://doi.org/10.1002/jclp.23797
Clinical Note: Research shows that rationally countering obsessive thoughts (cognitive restructuring) can inadvertently reinforce compulsive patterns by providing temporary reassurance. ERP promotes long-term cognitive flexibility.
Is there a safe way to discuss sexual intrusive thoughts with a therapist without judgment?
Yes. You will not shock us, and you will not be judged.
Sexual obsessions (including fears about sexual orientation, pedophilia, incest, or other taboo content) are well-documented OCD presentations. Therapists specializing in OCD understand these thoughts are a symptom of anxiety, not a reflection of your desires or character.
Why Disclosure is Safe Here:
Research shows that 35% of licensed psychologists misdiagnose Sexual Orientation OCD because they don’t understand the condition. At our Victoria BC practice, we specialize in OCD treatment, which means we recognise these thoughts as exactly what they are: intrusive, unwanted mental noise that OCD latches onto.
What You Can Safely Share:
- Intrusive thoughts about sexual acts that horrify you
- Fears that thoughts “mean” something about your sexuality or character
- Worries about acting on thoughts (even though you never would)
- Shame about having these thoughts
Your Privacy is Legally Protected:
As a Canadian Certified Counsellor (CCC) bound by CCPA ethics and BC’s PIPA, we cannot share what you tell us without your permission. Having intrusive thoughts does not meet any legal threshold for breaking confidentiality.
During your first session, we explain exactly how confidentiality works so you know what’s protected. You control the pace of disclosure and are never pressured to share more than feels safe.
It takes courage to ask for help with this. book a free consultation and let’s start breaking the cycle of shame together.
Evidence-Based Practice References
Weinberg, Lauren, Loni A. Martin, Kristin M. Post, and Emily J. Ricketts. “Psychologists’ Diagnostic Accuracy and Treatment Recommendations for Obsessive-Compulsive Disorder.” Journal of Clinical Psychology 81, no. 5 (2025): 324-333. https://doi.org/10.1002/jclp.23775
Intrusive Thoughts Therapy in Victoria | Judgment-Free Support
Am I crazy for having intrusive thoughts? Am I a bad person for my thoughts? If you are scared of your own thoughts or cannot stop wondering what if my intrusive thoughts are real, you are not losing your mind. You are experiencing something that clinical research shows affects 94 percent of the population. The difference is not having the thoughts; it is getting stuck in them.
Maybe your brain will not shut off. Maybe you cannot stop thinking about something no matter how hard you try. Maybe the thoughts are violent, sexual, or blasphemous, and the shame is unbearable. For people whose intrusive thoughts attach to faith; what clinicians call scrupulosity; the distress can feel like a spiritual crisis as much as a psychological one.
This includes what clinicians call harm OCD; unwanted thoughts about hurting yourself or someone you love, despite having no intention of doing so. It includes the call of the void; that inexplicable impulse when standing near a ledge or driving on a highway that you would never act on. These thoughts feel monstrous precisely because they go against everything you value. The distress is the proof that you care.
I’m Sean Lewis, a Canadian Certified Counsellor (CCC #11252849) with the CCPA, holding both a Master of Arts in Counselling Psychology and a Master of Divinity. That combination is rare and it matters here. My clinical training in Acceptance and Commitment Therapy (ACT) directly targets the relationship between you and your thoughts through a process called cognitive defusion; learning to observe thoughts without obeying them. My theological training means I can work with religious intrusive thoughts, blasphemous thoughts, and scrupulosity without dismissing your faith or pathologizing your beliefs. My military background provides understanding of hypervigilance-driven intrusive imagery in veterans and first responders.
ACT builds psychological flexibility; your ability to have a disturbing thought, recognise it as a thought, and still choose your next action based on your values rather than your fear. Mindfulness-based interventions support this work by creating distance between you and the noise in your head.
I offer intrusive thoughts therapy and rumination counselling in Victoria, BC, from my Colwood office in the Westshore, serving Langford and Greater Victoria, with virtual sessions across British Columbia. book a free consultation.
As a CCC through the Canadian Counselling and Psychotherapy Association, my counselling services qualify for extended health reimbursement under most benefit plans.