Trauma & PTSD Therapy
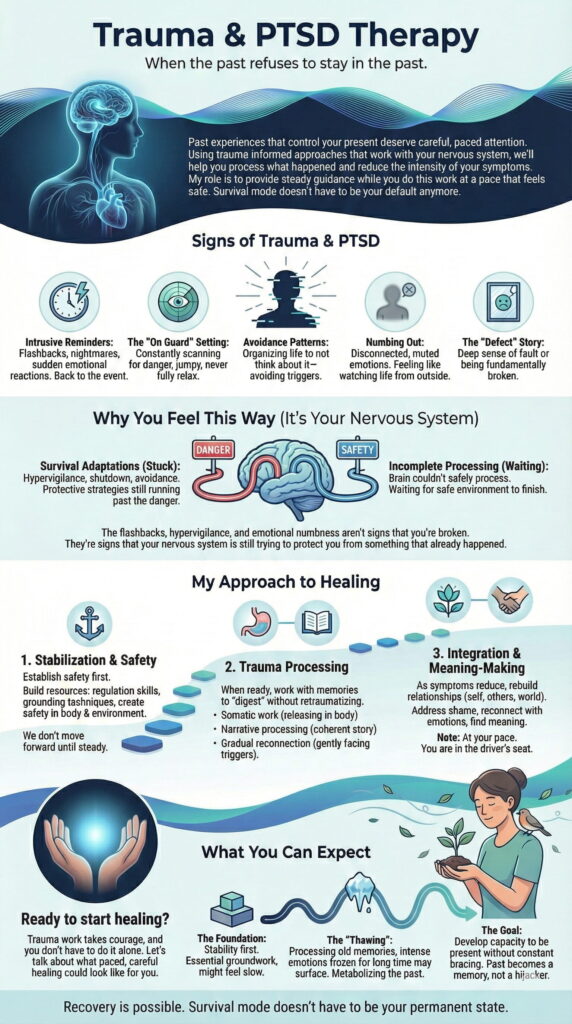
Signs of Trauma & PTSD
- Intrusive Reminders: Flashbacks, nightmares, or sudden emotional reactions that transport you back to the event. Something triggers you, and suddenly you aren’t in the present anymore.
- The “On Guard” Setting: You are constantly scanning for danger, jumping at sudden noises, unable to feel safe even in objectively safe environments. Your nervous system never fully relaxes.
- Avoidance Patterns: You organize your life around not thinking about what happened—avoiding people, places, conversations, or even emotions that might trigger memories.
- Numbing Out: You feel disconnected from yourself and others. Positive emotions are muted or absent. You might describe feeling like you’re watching your life from the outside.
- The “Defect” Story: You carry a deep sense that what happened was somehow your fault, or that you are fundamentally broken because of it.
Why You Feel This Way (It's Your Nervous System)
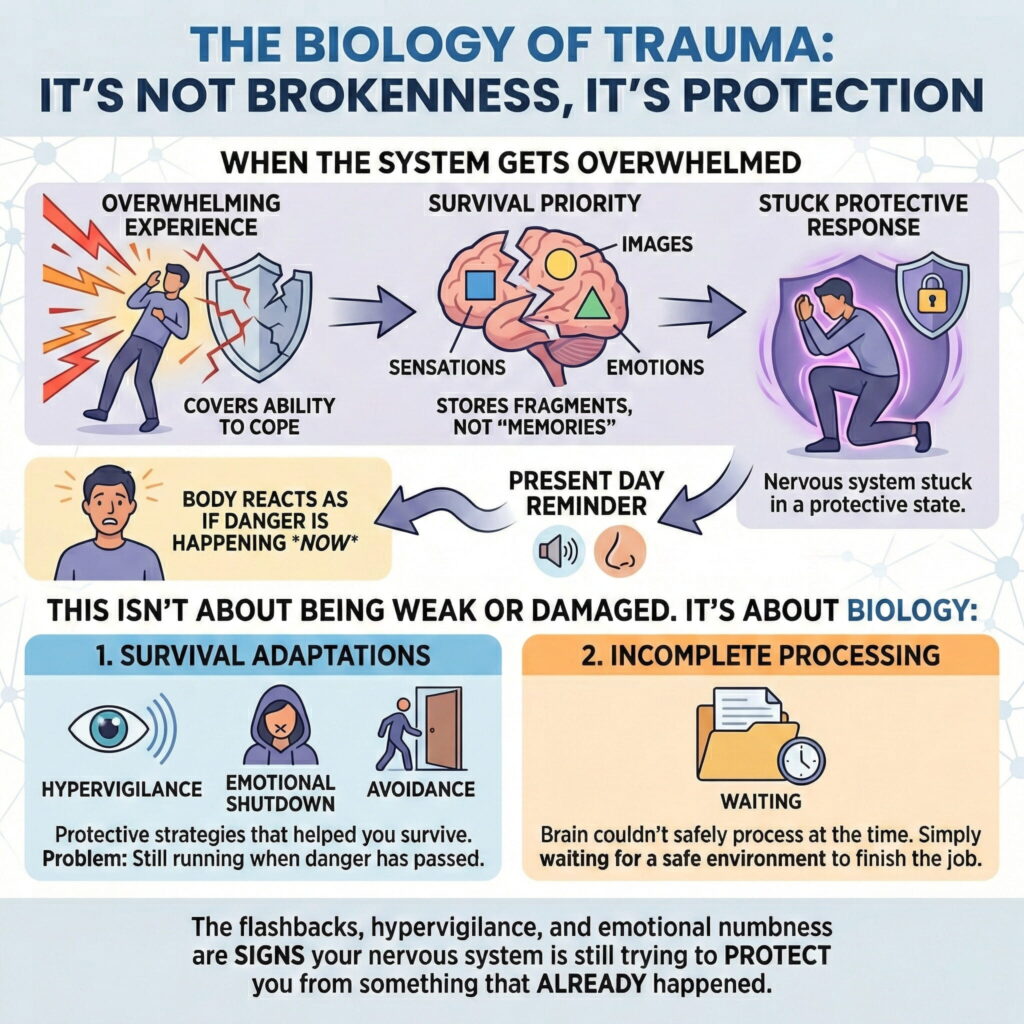
- Survival Adaptations: Hypervigilance, emotional shutdown, and avoidance were protective strategies that helped you survive. The problem is they’re still running even though the danger has passed.
- Incomplete Processing: Your brain couldn’t safely process the experience at the time. It’s simply waiting for a safe environment to finish the job.

My Approach to Healing
- Somatic work: Releasing trauma held in the body
- Narrative processing: Creating a coherent story so the memory feels like the past
- Gradual reconnection: Gently facing trauma-related triggers in a controlled, safe way to reclaim your freedom

Ready to Stop Surviving and Start Living?
Trauma keeps your body stuck in the past. Let's work at your pace to help you feel safe again.
$150 per 50-minute session - Insurance billing available
What You Can Expect
Healing from trauma isn’t a straight line. There will be progress, setbacks, and periods where it feels like nothing is changing.
The Foundation: We start with stability. This might feel slow, but it’s essential groundwork.
The “Thawing”: As we process old memories, you might feel emotions that have been frozen for a long time. This can be intense, but it’s a sign that your system is finally metabolizing what it couldn’t before. We’ll navigate this together.
The Goal: You won’t “delete” the memory, and you might always carry some sensitivity. But you’ll develop the capacity to be present in your life without constantly bracing for danger. The past becomes a memory, not something that hijacks your present.

Page Summary
References
National Institute of Mental Health. (2024, December). Post-traumatic stress disorder. https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd
Psychology Today. (n.d.). Complex PTSD. Retrieved January 28, 2026, from https://www.psychologytoday.com/basics/complex-ptsd
Frequently Asked Questions About Trauma Therapy
How do I know if I need trauma therapy or if my symptoms will go away on their own?
If trauma symptoms persist beyond one month, interfere with daily functioning, or worsen over time, therapy is strongly recommended. While some people naturally recover after traumatic events, early professional intervention reduces the risk of chronic PTSD and accelerates recovery.
The One-Month Rule
Immediately after trauma, it’s normal to experience sleep problems, heightened anxiety, intrusive memories, and emotional distress. This is your brain processing a threat; most people experience these reactions initially.
However, if symptoms persist or intensify beyond 30 days, professional help significantly improves outcomes. The DSM-5-TR diagnostic criteria distinguish between acute stress reactions (under 30 days) and PTSD (symptoms persisting beyond one month), specifically because the one-month threshold indicates when professional intervention becomes critical.
Signs You Need Trauma Therapy Now
Seek help if you’re experiencing:
Intrusive Symptoms:
- Unwanted memories, flashbacks, or nightmares about the trauma
- Physical reactions (racing heart, sweating) when reminded of the event
- Feeling like you’re reliving the trauma
Avoidance:
- Actively avoiding places, people, or activities connected to the trauma
- Avoiding thoughts or conversations about what happened
- Using substances to numb feelings
Mood & Thought Changes:
- Persistent negative beliefs (“I’m broken,” “The world is dangerous”)
- Emotional numbness or inability to feel positive emotions
- Memory gaps about important parts of the trauma
- Persistent fear, anger, guilt, or shame
Hyperarousal:
- Constant scanning for danger (hypervigilance)
- Exaggerated startle response
- Difficulty concentrating or sleeping
- Irritability or angry outbursts
Functional Impairment:
- Missing work or struggling with job performance
- Relationship conflicts or withdrawal from loved ones
- Neglecting responsibilities or self-care
A Common Pattern:
Lisa experienced a car accident. For the first two weeks, she had nightmares and avoided highways. Her doctor said, “Give it time; trauma reactions are normal.” Three months later, she was still having panic attacks while driving, avoiding all cars, and couldn’t get to work. She finally sought therapy and said, “I thought I should tough it out. I didn’t realize how stuck I was until I couldn’t function anymore.”
Why Early Intervention Matters
Avoidance strengthens fear. The more you avoid trauma reminders, the more your brain interprets them as genuinely dangerous. This creates a self-reinforcing cycle where avoidance brings temporary relief but long-term worsening.
Untreated trauma doesn’t fade; it generalizes. Initial triggers (specific locations, sounds, smells) expand to broader categories. Fear of one highway becomes fear of all driving. Distrust of one person becomes distrust of everyone.
Early therapy reduces the risk of chronic PTSD. Research shows that approximately 50% of people with acute stress reactions go on to develop chronic PTSD if left untreated. Early intervention significantly reduces this risk and prevents symptom escalation for many people.
When Symptoms May Resolve on Their Own
Some people naturally recover if they:
- Have strong social support and can talk about what happened
- Don’t develop persistent avoidance patterns
- Experience gradual, natural exposure to reminders without overwhelming distress
- Have no prior trauma history or mental health concerns
But even in these cases, therapy accelerates recovery and builds resilience against future stressors.
⚠️ WHEN TO SEEK HELP IMMEDIATELY
Contact crisis services right away if you’re experiencing:
- Plans of suicide or self-harm
- Plans to hurt yourself or others
- Inability to care for yourself or dependents
- Severe dissociation (feeling disconnected from reality)
- Psychotic symptoms (hallucinations, delusions)
Crisis Resources:
- Vancouver Island Crisis Line: 1-888-494-3888 (24/7)
- 9-8-8 Suicide Crisis Helpline: Call or text 988 (24/7)
- 911: For immediate danger
View complete crisis resources
The Bottom Line
Don’t wait to see if symptoms go away. Early intervention is more effective, requires fewer sessions, and prevents chronic PTSD. If you’re unsure whether you need help, a single consultation can clarify whether therapy would benefit you.
Ready to seek help? Book your first session to discuss with us what you need and we will help you get there.
Related Questions:
- What should I expect in a first trauma therapy session?
- How can therapy help with PTSD, and what is the healing process like?
- How long does trauma therapy take, and when will I start feeling better?
- When should I go to therapy?
Service Pages:
- Trauma & PTSD Therapy
- Anxiety Treatment
- Stress & Burnout
- Crisis & Safety Resources
Policy Details:
- Crisis Resources
- About Sean Lewis
Evidence-Based Practice References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.). Washington, DC: American Psychiatric Association, 2022\. \[DSM-5-TR diagnostic criteria for PTSD and Acute Stress Disorder\].https://doi.org/10.1176/appi.books.9780890425787
Bryant, R. A., Friedman, M. J., Spiegel, D., Ursano, R., & Strain, J. “Acute stress disorder in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).” In M. J. Friedman, T. M. Keane, & P. A. Resick (Eds.), Handbook of PTSD: Science and Practice (2nd ed., pp. 124-143). New York: Guilford Press, 2014\.
Karatzias, T. “Navigating the landscape of trauma treatments: the need for personalized care.” World Psychiatry 24, no. 1 (2025): 83-84. https://doi.org/10.1002/wps.21272
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. “Posttraumatic stress disorder in the National Comorbidity Survey.” Archives of General Psychiatry 52, no. 12 (1995): 1048-1060. https://doi.org/10.1001/archpsyc.1995.03950240066012
What should I expect in a first trauma therapy session?
Your first trauma therapy session focuses on safety, collaboration, and understanding, not processing the trauma itself. You won’t be asked to revisit traumatic memories in detail during your initial appointment.
What Actually Happens in Session One
Your first session is about building a foundation:
- Intake and Assessment: We discuss what brought you to therapy, current symptoms, and what you’re hoping to change
- Understanding Your Experience: You share as much or as little about your trauma as feels comfortable.
- Treatment Planning: We explore which therapeutic approaches align with your needs and comfort level
- Safety Establishment: We identify what helps you feel grounded and safe during sessions
Case Study (Composite scenario for educational purposes)
Marcus, a veteran, arrived for his first session visibly tense. He said, “I’m worried you’ll make me relive everything that happened overseas.” I explained that our first meeting was about understanding his current struggles—nightmares, hypervigilance, and avoiding crowds—not forcing him to recount traumatic details. We spent the session discussing his goals, what felt manageable, and building a collaborative treatment plan. He left saying, “I expected to be interrogated. Instead, I felt heard.”
What You’ll Be Asked:
- Current symptoms affecting your daily life (sleep, relationships, work)
- What you’re avoiding or what feels overwhelming
- Previous therapy experiences and what did or didn’t help
- Your preferences for how we work together
What You Won’t Be Asked:
- Detailed descriptions of traumatic events (unless you want to share)
- To make immediate commitments to exposure work
- To process memories before you’re ready
You’re in Control
First sessions establish that you decide the pace. Effective trauma therapy respects your autonomy; you’re never forced to discuss what feels unsafe. Many people worry therapy will make things worse before they get better, but evidence-based approaches prioritize stabilization before any deeper work.
Ready to take the first step? Book your initial consultation in Victoria, Langford, Saanich, the Westshore, or Sooke.
Related Questions:
- How do I know if I need trauma therapy or if my symptoms will go away on their own?
- Does trauma therapy require processing or revisiting the traumatic memory in detail?
- Can I tell my therapist anything?
- What types of counselling do you offer?
Service Pages:
- Trauma & PTSD Therapy
- Anxiety Treatment
- What is Acceptance and Commitment Therapy (ACT)?
Policy Details:
- Informed Consent for Therapy
- Privacy Policy & Confidentiality
- About Sean Lewis, MA, MDiv, CCC
Evidence-Based Practice References
Cloitre, M., Courtois, C. A., Charuvastra, A., Carapezza, R., Stolbach, B. C., & Green, B. L. “Treatment of complex PTSD: Results of the ISTSS expert clinician survey on best practices.” Journal of Traumatic Stress 24, no. 6 (2011): 615-627. https://doi.org/10.1002/jts.20697
Granner, J. R., & Seng, J. S. “Using Theories of Posttraumatic Stress to Inform Perinatal Care Clinician Responses to Trauma Reactions.” Journal of Midwifery & Women’s Health 66, no. 5 (2021): 567-578. https://doi.org/10.1111/jmwh.13287
Canadian Counselling and Psychotherapy Association (CCPA). “Code of Ethics (2020).” Article B9 “Confidentiality.” Ottawa: CCPA, 2020\. https://www.ccpa-accp.ca/wp-content/uploads/2020/05/CCPA-2020-Code-of-Ethics-E-Book-EN.pdf
Do I need a referral from my doctor to start trauma therapy?
No. You don’t need a doctor’s referral to access trauma therapy in British Columbia. You can book directly and start treatment immediately.
How It Works in BC
In BC, counselling services operate privately outside the public healthcare system. This means:
- No referral required: You can self-refer and book directly
- No waitlist: You’re not added to public mental health waitlists
- Faster access: First available appointment is often within 1-2 weeks
- You choose your therapist: You’re not assigned to whoever is available in the public system
When You WOULD Need a Referral
You only need a doctor’s referral if:
- You’re accessing publicly funded mental health services through Island Health or BC Mental Health & Substance Use Services (free but often 3-6 month waitlists)
- Your insurance requires a referral (rare; most extended health plans don’t require this for counselling)
Insurance & Referrals
Most extended health insurance plans in BC do NOT require referrals for mental health coverage. However, a few plans do. Check your benefits or ask:
“Do I need a doctor’s referral to access counselling benefits?”
If your plan requires one, your family doctor can write a simple referral noting you’re seeking counselling for trauma/PTSD.
Case Study (Composite scenario for educational purposes)
Nadia assumed she needed a referral. She waited 6 weeks to see her doctor, who then told her, “You don’t need a referral for private counselling. Just book directly.” She lost 6 weeks thinking she had to wait for permission.
The Advantage of Direct Access
Speed: Book online today, start therapy within days. Choice: Select a therapist specializing in trauma rather than being assigned to whoever’s available. Control: You set the pace and frequency; you’re not limited by public system constraints.
What About Psychiatrists or Psychologists?
- Psychiatrists: Require referrals from family doctors; typically 6-12 month waitlists in BC; focus on medication management
- Psychologists: No referral needed for private services; often $200-$250/session
- Registered Clinical Counsellors (RCC) / Canadian Certified Counsellors (CCC): No referral needed; $120-$180/session; provide evidence-based trauma therapy
All three can provide effective trauma treatment; the difference is cost, wait times, and whether you need medication.
Can My Doctor Help?
Your family doctor can:
- Provide a referral letter if your insurance requires one
- Prescribe medication if you’re interested in that option
- Rule out medical causes of symptoms (sleep disorders, thyroid issues)
But you don’t need to see your doctor before booking trauma therapy.
The Bottom Line
You can start trauma therapy today without a doctor’s referral. Simply book an appointment online and begin treatment immediately.
No referral needed. Book your first session now and start therapy this week.
Related Questions:
- How much does trauma therapy cost, and is it covered by insurance?
- How do I know if you’re qualified? (CCC credentials)
- What types of counselling do you offer?
Service Pages:
- Trauma & PTSD Therapy
- About Sean Lewis, MA, MDiv, CCC
Policy Details:
- Booking & Access
- Insurance Coverage
Evidence-Based Practice References
BC Association of Clinical Counsellors (BCACC). “Find a Counsellor.” Accessed February 2, 2026\. https://bc-counsellors.org/counsellors/
Canadian Counselling and Psychotherapy Association (CCPA). “Find a Counsellor.” Accessed February 2, 2026\. https://www.ccpa-accp.ca/find-a-counsellor/
How can therapy help with PTSD, and what is the healing process like?
Therapy for PTSD works by helping you process trauma, reduce avoidance, and rebuild a sense of safety. Healing isn’t about forgetting what happened; it’s about changing your relationship to the memories so they no longer control your life.
How Trauma Affects Your Brain
After trauma, your brain’s threat-detection system stays on high alert. Normal reminders: sounds, smells, places can trigger the same fear response you experienced during the actual threat. Your brain can’t tell the difference between “remembering danger” and “being in danger right now.”
The three core problems therapy addresses:
1. Intrusive Re-experiencing: Memories intrude when you don’t want them, often with the same emotional intensity as the original event 2. Avoidance: You avoid trauma reminders, which provides short-term relief but strengthens long-term fear 3. Altered Beliefs: You develop beliefs like “I’m not safe,” “I can’t trust anyone,” or “It was my fault”
What Therapy Actually Does
Acceptance and Commitment Therapy (ACT) for Trauma:
- Defusion: Learn to see traumatic thoughts and memories as mental events, not facts or threats
- Acceptance: Stop fighting or suppressing trauma responses; paradoxically, this reduces their intensity
- Values Clarification: Identify what matters most and take action aligned with your values, even when fear shows up
- Present-Moment Awareness: Build skills to ground yourself when flashbacks or panic arise
The result: Trauma memories lose their ability to hijack your life. You can acknowledge what happened without being controlled by it.
Case Study (Composite scenario for educational purposes)
David, a first responder, avoided driving past the intersection where he’d witnessed a fatal accident. Even thinking about that route triggered panic. Through ACT, he learned to notice the fear (“There’s that ‘danger’ thought again”), accept it without fighting it, and gradually return to driving because being a present father (his core value) mattered more than avoiding discomfort. The memory didn’t disappear, but it stopped controlling his choices.
The Healing Process: What to Expect
Early Phase (Sessions 1-4):
- Learning about trauma responses and why they make sense
- Building grounding and emotional regulation skills
- Clarifying treatment goals and your values
Middle Phase (Sessions 5-10):
- Practicing defusion and acceptance with trauma-related thoughts
- Gradually reducing avoidance behaviors
- Processing how trauma has affected your beliefs about safety, trust, and control
Later Phase (Sessions 10+):
- Consolidating gains and building resilience
- Addressing remaining stuck points
- Planning for maintaining progress after therapy ends
Common concerns about the process:
“Will therapy make me feel worse before I feel better?” Some distress is normal as you stop avoiding trauma-related emotions, but effective therapy doesn’t retraumatize you. We work at a pace you control, and you always have tools to manage distress.
“Will I have to relive the trauma?” With ACT, you don’t have to recount traumatic events in detail unless you choose to. Healing comes from changing how you relate to memories, not from forced exposure to them.
“How will I know if it’s working?” Early signs include: sleeping better, fewer panic attacks, returning to avoided activities, feeling more present with loved ones. Recovery isn’t linear; setbacks happen but become less frequent and less intense over time.
The Reality
Trauma recovery is hard work, but it’s also deeply empowering. You learn you can feel fear without being controlled by it, remember pain without reliving it, and move forward while honoring what happened.
Ready to start the healing process? Book your first session to work on PTSD using evidence-based approaches.
Related Questions:
- What types of therapy are most effective for PTSD or trauma?
- How long does trauma therapy take, and when will I start feeling better?
- Does trauma therapy require processing or revisiting the traumatic memory in detail?
Service Pages:
- Trauma & PTSD Therapy
- What is Acceptance and Commitment Therapy (ACT)?
- Mindfulness Therapy
Therapeutic Approach Pages:
- Acceptance and Commitment Therapy
- Cognitive Behavioural Therapy
Evidence-Based Practice References
Sciarrino, N. A., Warnecke, A. J., & Teng, E. J. “A Systematic Review of Intensive Empirically Supported Treatments for Posttraumatic Stress Disorder.” Journal of Traumatic Stress 33, no. 4 (2020): 443-454. https://doi.org/10.1002/jts.22556
Granner, J. R., & Seng, J. S. “Using Theories of Posttraumatic Stress to Inform Perinatal Care Clinician Responses to Trauma Reactions.” Journal of Midwifery & Women’s Health 66, no. 5 (2021): 567-578. https://doi.org/10.1111/jmwh.13287
Back, S. E., Jarnecke, A. M., Norman, S. B., Zaur, A. J., & Hien, D. A. “State of the Science: Treatment of comorbid posttraumatic stress disorder and substance use disorders.” Journal of Traumatic Stress 37, no. 6 (2024): 803-813. https://doi.org/10.1002/jts.23049
Does trauma therapy require processing or revisiting the traumatic memory in detail?
No. Effective trauma therapy does not require you to describe traumatic events in detail before you feel ready. Many evidence-based approaches help you manage PTSD symptoms without requiring you to recount what happened.
Different Approaches to Trauma Therapy
Trauma-Focused Therapies with Memory Processing:
Some trauma therapies—like Prolonged Exposure (PE) or Cognitive Processing Therapy (CPT)—involve gradually revisiting the traumatic memory to reduce fear and avoidance. These approaches have the strongest research evidence for PTSD treatment and are “strongly recommended” by the American Psychological Association.
How they work:
- Gradual, client-paced exposure to traumatic memories
- You control the pace; nothing is forced
- Helps your brain reprocess memories so they no longer feel dangerous
- Highly effective but can feel overwhelming for some people
Present-Focused Therapies (ACT, EMDR):
Other evidence-based approaches don’t require detailed recounting:
Acceptance and Commitment Therapy (ACT):
- Focuses on changing your relationship to traumatic memories, not eliminating them
- Teaches you to notice intrusive thoughts as “mental noise” rather than threats (cognitive defusion)
- Helps you accept difficult emotions rather than fighting them, which reduces struggle
- Emphasizes taking values-based action even while distress is present
- Research shows meaningful improvements in PTSD symptoms, though the evidence base is smaller than for PE/CPT
Case Study (Composite scenario for educational purposes)
Rebecca experienced childhood abuse. The thought of describing what happened made her physically ill. Her previous therapist used Prolonged Exposure, which she found too overwhelming and discontinued. With ACT, we worked on recognizing intrusive memories as mental events rather than current threats, accepting grief without suppression, and reconnecting with her children despite fear. She improved significantly without detailed memory recounting.
When Memory Processing May Be Helpful
For some people—especially those with intrusive flashbacks, persistent nightmares, or trauma-related beliefs (“It was my fault,” “I can’t trust anyone”)—working with the traumatic memory alongside a trained therapist can provide relief.
Memory processing can help:
- Reduce the frequency and intensity of intrusive re-experiencing
- Challenge stuck beliefs about the trauma
- Create a coherent narrative that makes sense of what happened
If memory processing becomes appropriate, we discuss that option together; you always control the pace.
The Bottom Line
You don’t have to describe traumatic events in detail to benefit from therapy. However, for some people with severe intrusive symptoms, memory processing can be helpful. We’ll collaborate to find the approach that fits your needs—whether that’s ACT, a trauma-focused approach like CPT, or a combination.
Interested in trauma therapy that respects your pace and preferences? Book a session to explore which approach is right for you.
Related Questions:
- What should I expect in a first trauma therapy session?
- How can therapy help with PTSD, and what is the healing process like?
- What types of therapy are most effective for PTSD or trauma?
Service Pages:
- Trauma & PTSD Therapy
- What is Acceptance and Commitment Therapy (ACT)?
- Anxiety Treatment
Therapeutic Approach Pages:
- Acceptance and Commitment Therapy
- Mindfulness Therapy
- Cognitive Behavioural Therapy
Evidence-Based Practice References
Lang, A. J., Schnurr, P. P., Jain, S., He, F., Walser, R. D., Bolton, E., Benedek, D. M., et al. “Randomized controlled trial of acceptance and commitment therapy for distress and impairment in OEF/OIF/OND veterans.” Psychological Trauma: Theory, Research, Practice, and Policy 9, no. S1 (2017): 74-84. https://doi.org/10.1037/tra0000127
Foa, E. B., Hembree, E. A., & Rothbaum, B. O. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences. New York: Oxford University Press, 2007\.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (2nd ed.). New York: Guilford Press, 2012\.
American Psychological Association. Clinical Practice Guideline for the Treatment of PTSD. Washington, DC: American Psychological Association, 2017\. https://www.apa.org/ptsd-guideline
Walser, R. D., & Westrup, D. Acceptance and Commitment Therapy for the Treatment of Post-Traumatic Stress Disorder and Trauma-Related Problems. Oakland, CA: New Harbinger Publications, 2007\.
Ehlers, A., & Clark, D. M. “A cognitive model of posttraumatic stress disorder.” Behaviour Research and Therapy 38, no. 4 (2000): 319-345. https://doi.org/10.1016/S0005-7967(99)00123-000123-0)
What types of therapy are most effective for PTSD or trauma?
The most effective treatments for PTSD are trauma-focused therapies including Cognitive Processing Therapy (CPT), Prolonged Exposure (PE), and Eye Movement Desensitization and Reprocessing (EMDR). These three approaches have the strongest research evidence, with 100+ randomized controlled trials each. Acceptance and Commitment Therapy (ACT) shows promising results with a smaller but growing evidence base.
Evidence-Based Approaches with Strong Research Support
Cognitive Processing Therapy (CPT):
- Helps you identify and change unhelpful beliefs about the trauma (“It was my fault,” “I can’t trust anyone”)
- Typically 12 sessions
- Focuses on “stuck points”—thoughts keeping you from recovering
- Research: 100+ randomized controlled trials; APA “Strongly Recommended”
- Best for: People who want to examine how trauma changed their beliefs
Prolonged Exposure (PE):
- Gradual, repeated exposure to trauma memories and avoided situations
- Typically 8-15 sessions
- Includes imaginal exposure (recounting trauma) and in vivo exposure (approaching avoided places/activities)
- Research: 100+ randomized controlled trials; APA “Strongly Recommended”
- Best for: People comfortable with memory processing and willing to face avoided situations
Eye Movement Desensitization and Reprocessing (EMDR):
- Uses bilateral stimulation (eye movements, taps) while processing trauma
- Typically 8-12 sessions
- Doesn’t require detailed verbal description of trauma
- Research: 50+ randomized controlled trials; APA “Strongly Recommended”
- Best for: People who find talk therapy difficult or want a less verbally intensive approach
These three approaches show equivalent effectiveness with large effect sizes. Research finds no significant differences in outcomes between CPT, PE, and EMDR.
Emerging Approach: Acceptance and Commitment Therapy (ACT)
Acceptance and Commitment Therapy (ACT):
- Teaches you to change your relationship to traumatic memories rather than eliminating them
- Focuses on living according to your values despite trauma-related discomfort
- Doesn’t require detailed memory processing
- Typically 12-16 sessions
- Research: 10-15 randomized controlled trials showing promising results; medium-to-large effect sizes
- Evidence base: Smaller than CPT/PE/EMDR but growing; not yet listed as “Strongly Recommended” by APA
- Best for: People who want to avoid detailed memory exposure or who’ve struggled with other approaches
Research by Lang and colleagues (2017) shows ACT produces meaningful improvements in PTSD symptoms, with effect sizes slightly smaller than exposure-based therapies but still clinically significant.
How They Compare
Side-by-Side Comparison
| Approach | Memory Processing Required? | Typical Length | Research Evidence | Key Focus |
|---|---|---|---|---|
| —– | —– | —– | —– | —– |
| CPT | Moderate (examining beliefs) | 12 sessions | 100+ RCTs; APA “Strongly Recommended” | Challenging stuck points |
| PE | High (detailed exposure) | 8-15 sessions | 100+ RCTs; APA “Strongly Recommended” | Habituation to fear |
| EMDR | Moderate (with bilateral stimulation) | 8-12 sessions | 50+ RCTs; APA “Strongly Recommended” | Reprocessing memories |
| ACT | Low (optional) | 12-16 sessions | 10-15 RCTs; Promising evidence | Values-based action |
Effectiveness:
- CPT, PE, EMDR: Equivalent large effect sizes; 60-65% of civilian patients no longer meet PTSD criteria after treatment
- ACT: Medium-to-large effect sizes; meaningful symptom improvement; slightly smaller evidence base
Case Study (Composite scenario for educational purposes)
Claire tried PE first but found recounting her assault repeatedly too overwhelming. She switched to ACT and learned to notice trauma memories as “mental events” rather than current threats, take valued action despite fear, and rebuild her life without forced exposure. She said, “PE felt like drowning. ACT taught me to swim.”
What About Regular Talk Therapy?
Generic “talk therapy” (non-trauma-focused counselling) is less effective for PTSD than the approaches above. While supportive therapy can help you feel heard, it doesn’t provide the specific skills and interventions needed to change trauma responses.
Trauma-focused therapy is directive and skill-based; you learn specific techniques to reduce symptoms and change how you relate to traumatic memories.
The Bottom Line
CPT, PE, and EMDR have the strongest research evidence for PTSD treatment, with equivalent effectiveness and 100+ studies each. ACT shows promising results with a smaller but growing evidence base, particularly for clients who prefer to avoid detailed memory work.
The most important factors for success are:
1. Therapist competence: Trained, experienced trauma therapists get better outcomes 2. Your engagement: Consistent attendance and homework practice matter more than modality 3. Therapeutic fit: Choose an approach that aligns with your preferences and comfort level
Interested in evidence based Trauma therapy? Book your first session to discuss begin your journey of healing.
Related Questions:
- How can therapy help with PTSD, and what is the healing process like?
- Does trauma therapy require processing or revisiting the traumatic memory in detail?
- How long does trauma therapy take, and when will I start feeling better?
- What’s the difference between types of therapy?
Service Pages:
- Trauma & PTSD Therapy
- What is Acceptance and Commitment Therapy (ACT)?
- Cognitive Behavioural Therapy
Therapeutic Approach Pages:
- Acceptance and Commitment Therapy
- Cognitive Behavioural Therapy
- Mindfulness Therapy
Evidence-Based Practice References
American Psychological Association. Clinical Practice Guideline for the Treatment of PTSD. Washington, DC: American Psychological Association, 2017\. https://www.apa.org/ptsd-guideline
Lang, A. J., Schnurr, P. P., Jain, S., He, F., Walser, R. D., Bolton, E., Benedek, D. M., et al. “Randomized controlled trial of acceptance and commitment therapy for distress and impairment in OEF/OIF/OND veterans.” Psychological Trauma: Theory, Research, Practice, and Policy 9, no. S1 (2017): 74-84. https://doi.org/10.1037/tra0000127
Granner, J. R., & Seng, J. S. “Using Theories of Posttraumatic Stress to Inform Perinatal Care Clinician Responses to Trauma Reactions.” Journal of Midwifery & Women’s Health 66, no. 5 (2021): 567-578. https://doi.org/10.1111/jmwh.13287
Norman, S. B. “Effectiveness of currently available psychotherapies for post-traumatic stress disorder and future directions.” World Psychiatry 21, no. 2 (2022): 309-310. https://doi.org/10.1002/wps.20974
Sciarrino, N. A., Warnecke, A. J., & Teng, E. J. “A Systematic Review of Intensive Empirically Supported Treatments for Posttraumatic Stress Disorder.” Journal of Traumatic Stress 33, no. 4 (2020): 443-454. https://doi.org/10.1002/jts.22556
Foa, E. B., Hembree, E. A., & Rothbaum, B. O. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences. New York: Oxford University Press, 2007\.
Resick, P. A., Monson, C. M., & Chard, K. M. Cognitive Processing Therapy for PTSD: A Comprehensive Manual. New York: Guilford Press, 2017\.
Shapiro, F. Eye Movement Desensitization and Reprocessing (EMDR) Therapy: Basic Principles, Protocols, and Procedures (3rd ed.). New York: Guilford Press, 2018\.
How long does trauma therapy take, and when will I start feeling better?
Most people notice initial improvement within 3 months, with significant symptom reduction typically occurring over 12-16 weekly sessions. However, trauma therapy timelines vary based on trauma complexity, symptom severity, and individual response.
Typical Timeline
Weeks 1-4: Stabilization & Skill-Building
- Learning about trauma responses and why they happen
- Building grounding techniques for managing flashbacks and anxiety
- Establishing safety and trust in the therapeutic relationship
- When you might notice change: Better sleep, reduced panic attacks
Weeks 5-12: Active Processing
- Working with traumatic memories (if using exposure-based therapy) or changing relationship to trauma (if using ACT)
- Reducing avoidance behaviors and expanding your life
- Addressing stuck points and unhelpful beliefs
- When you might notice change: Returning to avoided activities, feeling more present with loved ones, fewer intrusive thoughts
Weeks 12-16: Consolidation
- Strengthening gains and building resilience
- Addressing remaining symptoms
- Planning for maintaining progress after therapy ends
- When you might notice change: Engaging fully in life again, trauma no longer dominating your thoughts
Research-Based Expectations
- 3 months: Most clinicians expect initial good response within this timeframe
- 12-16 sessions: Standard evidence-based protocols typically run this length
- 60-65% of civilian PTSD patients: No longer meet diagnostic criteria after treatment
- 44% of veteran/military PTSD patients: No longer meet criteria (veterans often have more complex presentations)
Case Study (Composite scenario for educational purposes)
Tom, a paramedic with PTSD, said after 6 sessions: “I’m sleeping better and having fewer nightmares, but I still avoid ambulances and get panic attacks at work.” By session 12, he was back at work part-time. By session 16, he said, “The memories still come up, but they don’t control me anymore. I can do my job again.”
What Affects Timeline?
Faster progress typically happens when:
- Single-event trauma (one car accident) vs. complex trauma (childhood abuse)
- Strong social support
- No active substance use
- Engagement with homework/practice between sessions
Longer treatment may be needed for:
- Multiple traumatic events or chronic trauma
- Co-occurring depression, substance use, or other mental health concerns
- Limited support systems
- Ongoing stressors (unsafe living situation, legal issues)
When Progress Feels Slow
Recovery isn’t linear. You might feel significantly better, then have a setback after a trigger or anniversary. This doesn’t mean therapy isn’t working; it means your nervous system is still learning new patterns.
Common concerns:
“It’s been 8 sessions and I still have nightmares.”
Nightmares often persist longer than other symptoms but typically decrease in frequency and intensity. By session 12-16, most people report significant improvement.
“I feel worse than when I started.”
Early sessions can temporarily increase distress as you stop avoiding trauma-related emotions. This usually resolves within 4-6 sessions as you build skills to manage distress.
“Will I ever be fully ‘cured’?”
PTSD treatment aims for symptom reduction and functional improvement, not erasing memories. Most people reach a point where trauma no longer significantly impairs their life, even if occasional reminders cause discomfort.
Intensive Options
Some treatment programs offer intensive (daily or multiple sessions per week) therapy, which can condense 12-16 sessions into 2-3 weeks. Research shows intensive programs are highly effective with low dropout rates.
The Bottom Line
Most people begin noticing improvements within the first few months. Full recovery typically takes 3-6 months of weekly therapy, though complex cases may require longer. The key is consistent engagement; therapy works when you show up and practice skills between sessions.
Ready to start your recovery timeline? Book your first session to begin evidence-based trauma therapy.
Related Questions:
- How can therapy help with PTSD, and what is the healing process like?
- What types of therapy are most effective for PTSD or trauma?
- How do I know if I need trauma therapy or if my symptoms will go away on their own?
Service Pages:
- Trauma & PTSD Therapy
- Anxiety Treatment
Evidence-Based Practice References
Norman, S. B. “Effectiveness of currently available psychotherapies for post-traumatic stress disorder and future directions.” World Psychiatry 21, no. 2 (2022): 309-310. https://doi.org/10.1002/wps.20974
Cloitre, M., Courtois, C. A., Charuvastra, A., Carapezza, R., Stolbach, B. C., & Green, B. L. “Treatment of complex PTSD: Results of the ISTSS expert clinician survey on best practices.” Journal of Traumatic Stress 24, no. 6 (2011): 615-627. https://doi.org/10.1002/jts.20697
Sciarrino, N. A., Warnecke, A. J., & Teng, E. J. “A Systematic Review of Intensive Empirically Supported Treatments for Posttraumatic Stress Disorder.” Journal of Traumatic Stress 33, no. 4 (2020): 443-454. https://doi.org/10.1002/jts.22556
Hamblen, J. L., Grubbs, K. M., Cole, B., Schnurr, P. P., & Harik, J. M. “”Will it work for me?” Developing patient-friendly graphical displays of posttraumatic stress disorder treatment effectiveness.” Journal of Traumatic Stress 35, no. 3 (2022): 999-1010. https://doi.org/10.1002/jts.22808
How much does trauma therapy cost, and is it covered by insurance?
Sessions cost $150 for 50 minutes, and most extended health insurance plans cover therapy with a Canadian Certified Counsellor (CCC). Many people pay nothing out-of-pocket if their plan includes mental health benefits.
Insurance Coverage
As a Canadian Certified Counsellor through the Canadian Counselling and Psychotherapy Association (CCPA), my services are eligible for reimbursement under most extended health plans in BC. Coverage varies by plan, but typical benefits include:
Common Coverage Amounts:
- $500-$3,000 per year for counselling services
- Some plans cover up to 80-100% of session costs
- Coverage may be listed as “Psychologist,” “Counsellor,” “Registered Clinical Counsellor (RCC),” or “Mental Health Practitioner”
How to Check Your Coverage:
1. Call your insurance provider 2. Ask specifically: “Do you cover Canadian Certified Counsellors (CCC) or Registered Clinical Counsellors?” 3. Confirm: Annual maximum, percentage covered, and whether you need a referral
Payment Process
You pay at the time of service: Sessions are $150 (50 minutes), payable by e-transfer, credit card, cash, or cheque.
You submit for reimbursement: I provide detailed receipts you submit to your insurance company. Most insurers reimburse within 1-2 weeks.
Some plans offer direct billing: If your plan allows, I can submit claims directly so you don’t pay upfront.
What if I Don’t Have Insurance?
Payment plans: We can discuss spreading costs across sessions if paying $150 upfront creates hardship.
EAP programs: Some employers offer Employee Assistance Programs (EAP) providing 3-8 free sessions; check with your HR department.
Sliding scale (limited availability): I reserve a small number of sliding-scale spots for clients experiencing significant financial barriers.
Comparing Costs
Not seeking treatment costs more:
- Lost productivity due to PTSD: Studies estimate $3,000-$10,000 annually
- Relationship breakdowns, job loss, substance use: Far exceed therapy costs
- Chronic PTSD requiring years of treatment: More expensive than 12-16 sessions addressing it early
The Investment
Trauma therapy typically requires 12-16 sessions ($1,800-$2,400 total). With insurance covering 80%, your out-of-pocket cost might be $360-$480. This investment in your mental health pays dividends in improved functioning, relationships, and quality of life.
Ready to use your benefits? Book a session and I’ll provide receipts for insurance reimbursement.
Related Questions:
- Do I need a referral from my doctor to start trauma therapy?
- How do I know if you’re qualified? (CCC credentials)
- What types of counselling do you offer?
Service Pages:
- Trauma & PTSD Therapy
- Insurance & Payment Information
- About Sean Lewis, MA, MDiv, CCC
Policy Details:
- Fees & Payment
- Insurance Coverage
Evidence-Based Practice References
Canadian Counselling and Psychotherapy Association (CCPA). “CCC Designation.” Accessed February 2, 2026\. https://www.ccpa-accp.ca/ccc/
BC Association of Clinical Counsellors (BCACC). “Registered Clinical Counsellor Designation.” Accessed February 2, 2026\. https://bc-counsellors.org/counsellors/
Is medication necessary for PTSD, or can therapy alone help?
Psychotherapy alone is highly effective for PTSD and is the recommended first-line treatment. While medication can be helpful as an addition to therapy for some people, you don’t need to take medication to recover from trauma.
What Clinical Guidelines Recommend
The 2023 U.S. Department of Veterans Affairs and Department of Defense (VA/DoD) Clinical Practice Guideline for PTSD provides clear recommendations:
Strongly Recommended (First-Line):
- Individual trauma-focused psychotherapies (Prolonged Exposure, Cognitive Processing Therapy)
Conditionally Recommended (Second-Line or Adjunct):
- SSRIs/SNRIs (sertraline, paroxetine, venlafaxine) as addition to therapy or when therapy unavailable
The guideline explicitly recommends psychotherapy over medication as first-line treatment.
What the Research Shows
Research comparing psychotherapy and medication outcomes:
Trauma-Focused Psychotherapy:
- 60-65% of civilian patients no longer meet PTSD criteria after treatment
- 44% of veteran/military patients no longer meet criteria (veterans often have more complex presentations)
- Large effect sizes maintained at follow-up
- Skills learned continue benefiting patients after treatment ends
SSRIs/SNRIs (Medication):
- Studies show moderate symptom reduction
- Effects often diminish when medication is discontinued
- No skills learned for managing future stressors
- Side effects can include sexual dysfunction, weight changes, sleep disturbance
Important Context: Direct comparisons are difficult because medication studies typically involve different populations and don’t always include concurrent therapy. The most effective treatment for severe, complex PTSD is often trauma-focused therapy with medication added as needed.
When Medication Might Help as an Adjunct
Medication may be beneficial in addition to therapy if:
- Severe depression co-occurs with PTSD
- Panic attacks or severe anxiety interfere with daily functioning
- Sleep disturbance is severe and impairs therapy engagement
- You’ve started therapy and need additional support for symptom management
- Access to trauma-focused therapy is limited or delayed
Important: Medication doesn’t replace therapy. It can reduce symptom intensity, making it easier to engage in therapy work, but it doesn’t teach you skills to process trauma or change avoidance patterns.
Case Study (Composite scenario for educational purposes)
Angela’s doctor prescribed sertraline for PTSD after a sexual assault. After 8 weeks, her overall distress level decreased slightly, making it easier to get out of bed, but she still avoided dating, struggled with nightmares, and felt hypervigilant. She started therapy and learned skills to process trauma, reduce avoidance, and rebuild safety. She later said, “The medication helped stabilize my mood enough to do the therapy work. Therapy taught me how to live again.”
The Advantage of Therapy Alone
Skills last beyond treatment: Therapy teaches you strategies you carry forward; medication effects end when you stop taking it.
No medication side effects: Trauma therapy has no sexual dysfunction, weight gain, sleep changes, or other medication side effects.
Addresses root causes: Therapy changes how you process trauma and respond to triggers; medication only manages symptoms.
Research on Combined Treatment
Studies examining therapy plus medication versus therapy alone show:
- Combined treatment doesn’t significantly improve outcomes over therapy alone for most people
- Medication may help initial stabilization for severe symptoms
- Once stabilized, therapy drives the actual recovery process
Exception: For severe depression co-occurring with PTSD, combined treatment may be more effective initially.
If You’re Already on Medication
If you’re currently taking medication for PTSD:
- That’s fine; therapy will still work effectively
- Don’t stop medication without consulting your prescribing physician
- Many people successfully taper off medication after completing trauma therapy (with medical supervision)
- Therapy teaches skills that medication alone cannot provide
The Bottom Line
You don’t need medication to recover from PTSD. Trauma-focused psychotherapy is the most effective first-line treatment and should be your primary intervention. If medication would help you engage in therapy or manage severe symptoms, it can be added as an adjunct. But therapy—not medication—is what creates lasting change.
Want to explore therapy as your primary treatment? Book your first session to work on trauma using evidence-based approaches.
Related Questions:
- How can therapy help with PTSD, and what is the healing process like?
- What types of therapy are most effective for PTSD or trauma?
- How long does trauma therapy take, and when will I start feeling better?
- What’s the difference between a counsellor and a psychiatrist?
Service Pages:
- Trauma & PTSD Therapy
- Depression & Mood
- Anxiety Treatment
Evidence-Based Practice References
U.S. Department of Veterans Affairs and U.S. Department of Defense. “VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder (Version 4.0).” Washington, DC: Veterans Health Administration and Department of Defense, 2023\. https://www.healthquality.va.gov/guidelines/MH/ptsd/
Hamblen, J. L., Grubbs, K. M., Cole, B., Schnurr, P. P., & Harik, J. M. “”Will it work for me?” Developing patient-friendly graphical displays of posttraumatic stress disorder treatment effectiveness.” Journal of Traumatic Stress 35, no. 3 (2022): 999-1010. https://doi.org/10.1002/jts.22808
Burton, M. S., Marks, E. H., Bedard-Gilligan, M. A., Feeny, N. C., & Zoellner, L. A. “The effect of perceived life stress on posttraumatic stress disorder treatment outcome.” Journal of Traumatic Stress 34, no. 6 (2021): 1219-1227. https://doi.org/10.1002/jts.22744
Watts, B. V., Schnurr, P. P., Mayo, L., Young-Xu, Y., Weeks, W. B., & Friedman, M. J. “Meta-analysis of the efficacy of treatments for posttraumatic stress disorder.” Journal of Clinical Psychiatry 74, no. 6 (2013): e541-e550. https://doi.org/10.4088/JCP.12r08225
Rauch, S. A., Kim, H. M., Venners, M. R., Porter, K. E., Norman, S. B., Simon, N. M., Rothbaum, B. O., et al. “Change in posttraumatic stress disorder-related thoughts during treatment: Do thoughts drive change when pills are involved?” Journal of Traumatic Stress 35, no. 2 (2021): 496-507. https://doi.org/10.1002/jts.22762
What is a trauma trigger, and how do I recognize what is triggering my symptoms?
A trauma trigger is anything—a sight, sound, smell, situation, or internal sensation—that reminds your brain of the traumatic event and activates a fear response as if the threat is happening right now. Learning to identify your triggers is the first step toward managing them.
How Triggers Work
During trauma, your brain creates associations between the threat and everything happening around it. Later, when you encounter something similar, your nervous system reacts with the same intensity as during the original event—even though you’re objectively safe.
Your brain doesn’t distinguish between “remembering danger” and “being in danger.” This is why triggers produce real physical symptoms: racing heart, sweating, panic, or the urge to flee.
Common Types of Triggers
External (Sensory) Triggers:
- Sights: Places, people, or objects connected to the trauma
- Sounds: Loud noises, sirens, voices, music
- Smells: Specific scents (cologne, smoke, food)
- Physical sensations: Being touched in certain ways, specific body positions
Internal (Emotional/Cognitive) Triggers:
- Emotions: Feeling helpless, vulnerable, or out of control
- Thoughts: “What if it happens again?” or intrusive memories
- Body sensations: Elevated heart rate, tension, or fatigue
Situational Triggers:
- Anniversaries: Dates connected to the trauma
- Similar situations: Crowded places if trauma occurred in crowds; driving if trauma involved a car accident
Case Study (Composite scenario for educational purposes)
After a sexual assault, Maria was triggered by:
- The cologne her attacker wore (smell)
- Being in enclosed spaces with men (situational)
- Feeling helpless in other contexts, even unrelated to trauma (internal)
- The anniversary date each year (temporal)
She didn’t realize these were triggers at first; she just knew she’d suddenly feel panicked “for no reason.” Tracking patterns helped her identify what was activating her nervous system.
How to Identify Your Triggers
Track your reactions: When you notice sudden anxiety, flashbacks, or physical symptoms, ask:
- What was I doing right before this started?
- What did I see, hear, smell, or feel?
- What was I thinking about?
Look for patterns: Triggers often repeat. If you panic every time you drive past a specific intersection, or feel anxious when approached from behind, those are likely triggers.
Consider timing: Do symptoms worsen around anniversaries, specific times of day, or during certain activities?
Why Identifying Triggers Matters
Triggers feel random and uncontrollable when you don’t understand them. Once you identify patterns, you can:
- Predict when you might feel activated
- Prepare coping strategies in advance
- Gradually reduce avoidance and reclaim your life
What to Do When Triggered
Grounding techniques:
- 5-4-3-2-1: Name 5 things you see, 4 you hear, 3 you can touch, 2 you smell, 1 you taste
- Deep breathing: Slow, diaphragmatic breaths to calm your nervous system
- Remind yourself: “This is a memory. I am safe right now.”
Self-compassion: Triggers aren’t weakness or failure; they’re your brain trying to protect you based on past danger.
Therapy helps: ACT, CPT, and other trauma-focused approaches teach you to respond to triggers differently so they lose power over time.
TRIGGER SAFETY DISCLAIMER
If you experience a severe trigger that leaves you:
- Unable to ground yourself or return to the present
- Experiencing prolonged dissociation or flashbacks
- Having thoughts of self-harm
Consider contacting crisis support:
- Vancouver Island Crisis Line: 1-888-494-3888 (24/7)
- 9-8-8 Suicide Crisis Helpline: Call or text 988 (24/7)
- 911: For immediate danger
View complete crisis resources
The Goal Isn’t to Eliminate All Triggers
You can’t predict or avoid every possible reminder. The goal is to change how you respond to triggers so they no longer control your life. With therapy, most people find triggers become less intense, less frequent, and more manageable.
Ready to understand and manage your triggers? Book a session to work on trauma using evidence-based approaches.
Related Questions:
- How can therapy help with PTSD, and what is the healing process like?
- What types of therapy are most effective for PTSD or trauma?
- How do I know if I need trauma therapy or if my symptoms will go away on their own?
Service Pages:
- Trauma & PTSD Therapy
- Anxiety Treatment
- Mindfulness Therapy
- Crisis & Safety Resources
Therapeutic Approach Pages:
- Acceptance and Commitment Therapy
- Mindfulness Therapy
Evidence-Based Practice References
Mojallal, M., Simons, R. M., Simons, J. S., & Swaminath, S. “Daily exposure to combat-related cues and posttraumatic stress symptoms among veterans: Moderating effects of peri- and postdeployment experiences.” Journal of Traumatic Stress 37, no. 1 (2023): 57-68. https://doi.org/10.1002/jts.22991
Reeves, J. W., & Fisher, A. J. “An Examination of Idiographic Networks of Posttraumatic Stress Disorder Symptoms.” Journal of Traumatic Stress 33, no. 1 (2020): 84-95. https://doi.org/10.1002/jts.22491
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.). Washington, DC: American Psychiatric Association, 2022\.
Trauma Therapy in Victoria, BC | A Counsellor Who Has Lived It
If you have ever thought “why can’t I just get over it,” you are not broken; you are carrying something your nervous system has not finished processing. Maybe you get triggered but do not know why. Maybe it feels like it just happened even though it was years ago.
Sean Lewis served in the Canadian Armed Forces infantry. He does not need you to explain what hypervigilance feels like, or why asking for help can feel like a failure of character. His six years leading the Mustard Seed Street Church in Victoria gave him direct experience sitting with people whose trauma came from violence, homelessness, and systems that failed them.
As a trauma therapist in Victoria, BC, Sean works primarily through Acceptance and Commitment Therapy (ACT), which peer-reviewed research supports as an effective treatment for PTSD and operational stress injuries. ACT builds psychological flexibility rather than forcing you to relive painful experiences before you are ready.
Whether your trauma comes from service, childhood, relationships, or something you are still trying to name, Sean offers PTSD counselling in Colwood and the Westshore, with virtual trauma therapy across British Columbia. His counselling is covered by most extended health plans through the CCPA. Book a session.